I’ve found that one of the best ways to think is to write. Writing is thinking. This is why I sink so much time into writing this damned blog: To think my way through questions. It seems to work, though my conclusions aren’t always right.
To date I have been diagnosed with basil cell cancer, two squamous cell cancers and prostate cancer. What I have learned is what others have said all along- cancer is often a long-term affliction rather than an immediate death sentence. I’m in remission 4 times over.
Most of the time it is hard to appreciate simple and routine activity. The pertinent example here is how, during the process of chewing and swallowing food, we shift food around in our mouths with our tongues and use other musculature we are ordinarily unaware of. This is true for solid food and liquids. Highly automatic activity that we rarely think about. Then one fine day we can lose much of our ability to chew and swallow. I recently had that fine day.
Aspects of chewing and swallowing are two parts of our anatomy rarely considered: The epiglottis and the uvula. Radiation has damaged a swath of tissues and neck surgery has disrupted nerves that control of these two throaty bits of tissue. In 2013 I had a cumulative radiation dose of about 50 Gray to my neck in 1.8 Gray doses over 4 weeks. The Gray is a unit equal to 1.0 Joule of energy absorbed in 1.0 kilogram of tissue. Your onco-doc will prescribe a daily and cumulative dosage to a specific 3-dimensional section of tissue. The damage to tissue that radiation produces is grossly similar to sunburn (which is also radiation damage), but to the entire volume the beam passes through.
A digression into radiation
The clever machine that delivers the therapeutic x-radiation is called an IMRT- Intensity Modulated Radiation Therapy. It has an electron accelerator that slams high speed electrons into an angled copper target which causes the electrons to abruptly lose energy in the form of x-radiation. Prior to every treatment the tattoos on the patient are aligned with external laser beams and then an x-ray CT scanner mounted on the IMRT rotates around the patient lying on an adjustable table. This is to assure that the patient is properly placed for the IMRT to dose the desired volume yet limit the radiation dose to surrounding tissue.
What is the difference between x-radiation and gamma radiation? Gamma photons are much higher in energy and are ejected by the atomic nucleus. When the nucleus undergoes a transition from a higher energy state to a lower energy state, the conserved energy is ejected as a gamma photon. Often time when a nucleus undergoes a nuclear transition by particle emission or fission of the nucleus, the remaining nucleus is not at the lowest energy level possible and is metastable. Over time the nucleus can drop to the ground state energy, emitting a gamma photon. The gamma emission can be prompt or not.
X-rays result from an inner orbital electron being ejected by collisions with impinging outside electrons to leave a partially empty low energy orbital which is immediately refilled by upper level, higher energy electrons dropping to a lower energy orbital and conserving the energy change by emission of what we call an x-ray. There does not seem to be a sharp energy dividing line between x-rays and gamma rays.
The latest tumor
If you knew me anytime before September of this year, you’ll note that I spoke normally, absent slurs or other speech impediments. Today I speak with a distinct slur when attempting to speak certain sounds like s, ch, sh and words. I am as yet unable to lick my lips or stick out my tongue. You know that smacking sound you make while giving a short kiss? That’s gone too.
In August 2025 I was diagnosed with having a tumor on the left side of my tongue. Two years earlier what was to become a tumor was just a dysplasia and it was removed surgically. In September of this year, I had the tumor removed as a slice off the side of my tongue the width and thickness of a dime during a partial glossectomy procedure.
Another brief digression
In our college library during grad school, I would check the book carts to see if the book I sought hadn’t been shelved yet. One day while perusing the book cart I found a medical school text on maxillofacial surgery (1960’s). Being a curious person, I picked it up and thumbed through it. I was shocked and sickened to the point of hurling by what I saw. For the first time ever I had to run immediately to the restroom to vomit. Never again did I look into this topic.
The maxillofacial textbook detailed surgical techniques, the results of large-scale removal of large facial sections and underlying bone structures, and facial protheses. This often-left gaping, gruesome holes in the faces of patients, revealing parts of the anatomy never meant to be on display.
Circling back
So, imagine my dismay when, in 2013, I was diagnosed with stage 4 throat cancer. Then again 2 months ago I had another squamous cell tumor pop up on my tongue. Images of the maxillofacial textbook came back afresh. The throat cancer was HPV-induced and highly treatable but the tongue cancer was not, so they were not considered to be related.
My guess is that, of the 4 different cancers I have, the cancer that sends me into the crematory will likely be the stage 4 prostate cancer. My quest to remain above the grass will be at an end.
From all of this I have learned that swallowing difficulties with food inhalation can lead to pneumonia. My pneumonia wasn’t horrible, but it kills a lot of senior citizens. It’s been called something like the “the old man’s friend” since it can sometimes lead to a softer death.
The immediate effect that a cancer diagnosis has on most folks is to believe that you’re a dead-person-walking. Sometimes true, but not always. I’m in remission 4 times over. I’m always amused when at the dentist they put a radiation shield over me to get a low dose dental x-ray. Big whoop. A dose of 20 Gray all at once is considered to be an LD50 dose. Since 2013 I’ve absorbed over 100 Gray between 3 separate x-ray therapy treatments, two PET scans, and multiple CT scans too numerous to mention.
One final paragraph. While taking chemotherapy in 2013 for throat cancer, I spent 6 sessions in the infusion ward with cisplatin dripping into my vein. My chemo experience never had an adverse effect on me. However, each visit there were women a few seats away with breast cancer, presumably, getting their chemo. Often they were moaning and vomiting in heartbreaking discomfort. It was a picture of what some unfortunate folks have to endure, and I felt guilty about the ease with which I was receiving chemo. So far, I have been very, very lucky.
The months of August and September of this year, 2025, have been less than fun. I had a tumor removed from my tongue (a partial glossectomy) in August and a neck dissection in September to look for signs of spread. The 15 or so lymph nodes removed were all clear of cancer. As a result, my ability to swallow is impaired and my speech is now slurred. The dissection resulted in nerve damage resulting in malfunction of facial muscles and the ability of my tongue to participate normally in chewing and swallowing. You know that smacking sound you make when you kiss someone? That is now gone.
Combined with a previous problem with balance, I can easily appear as though I’m drunk or stoned. My nightmare is that I’ll end up doing a roadside sobriety test and fail it spectacularly. The copper will be momentarily satisfied that he/she found another drunk driver until I blow a 0.000 % on their handy-dandy blood alcohol meter. Yeah, then we’ll share some laughter together until I say ‘I told you so’ then we’ll part ways.
I disclose this personal information only to ask the broader question of who thinks of having a tumor cut out of your tongue when you’re younger? The inside of your mouth is perhaps the most intimate place on your body. Our consciousness is certainly tied in closely. It began as a small dysplasia which I had removed several years ago. This year it had regrown into a tumor, as dysplasia often does.
I’ve had difficulty choking on food since my throat cancer was heavily irradiated in 2013. But this new problem is more difficult and immediate. Eating and drinking normally causes food to come out my nose with prolonged coughing. Everything I eat must either be normally thick, like soup, or be thickened with carrageenan gum. Low viscosity fluids like water or soft drinks cause choking.
My ENT suggested physical therapy to help with the neck swelling through massage, but I said I just had to find a strip mall with a massage parlor. A moment of whimsy in the exam room.
This afternoon I’ll top off this surgery season with a root canal and crown. Happy happy joy joy. As a side note, Medicare has been surprisingly easy to work with.
First let me say that I have never been a smoker, drug user or sun bather. As a chemist I have always been cautious about chemical exposure. I have numerous cancers now with the two serious ones in remission. The new ones- who knows.
I use a university hospital and have been visited by flocks of med students looking at me in wonder, sometimes looking down my throat. I get a kick out of it. I always try to joke with them. All cancer diagnoses go before a faculty tumor board for collective assessment. That in particular drew me to this hospital.
My experience with numerous radiation, medical, ENT, and head & neck oncologists is that they absolutely do not want to discuss end of life issues. Maybe that is because I’m not near the end yet, though. But more likely they have production quotas and need to stick to the timeline. My head and neck oncologist did say that they were trying to keep me above the grass, though. That was cheerful.
Since July 22 of this year, I’ve had a partial glossectomy to remove a tumor resulting in a nickel-sized piece of the left edge of my tongue being removed, my first colonoscopy, a neck dissection looking for more cancer, and tomorrow is a root canal. Sonofabitch!
The glossectomy resulted in giving me slurred speech and then the neck dissection made it much worse with the added joy of serious swallowing difficulty. Liquids must be thickened with carrageenan gum to mostly avoid inhalation of food and drink. I’ve already been hospitalized with pneumonia resulting from inhaled food.
My 68th birthday was last week and while I received my well wishes, not a single person was moved to suggest a gerontologist, elder care facility or even as little as when the word “elderly” is used. I’m left up in the air …
It never occurred to me earlier in life that a piece of my tongue could be sliced out. What part of your body is more intimate in your daily consciousness than your mouth? I’ve had surgeons say “give me control of your tongue”. A fella doesn’t hear that very often.
The colonoscopy revealed 2 polyps suspected of being cancerous. So, to tally up the score, I have stage 4 prostate cancer, stage 4 throat cancer, tongue cancer, basil cell skin cancer, and possible colon cancer. Jesus H. Christ!! What next?.
The radiation of my throat resulted in the loss of about 1/2 of my salivary glands and taste buds. I’ve had dry mouth since radiation treatment in 2013, resulting in the loss of numerous teeth.
I was given radiation treatment of my prostate in 2014 and again last summer when the PSA score breached the 4.0 level. Since the 2014 treatment the thinking has changed on radiation dosage. Previously I was given about 1.8 Gray per dose. This time it was 5.0 Gray per dose over fewer doses. The thinking is that it is better to try to break the cancer cell DNA in 2 places at once rather than in just one place. In two rounds of x-radiation treatment of my prostate, I have experienced no pain or discomfort. I’ve had two rounds of 18F-Glucose injections for PET/CT scans.
The throat radiation was a different story. It gave me the world’s worst sore throat. I was fed through a stomach tube and was on opioids for an extended period. Let me say that I detest opioids and the constipation they bring. How do opioid addicts deal with this??
The throat cancer was from the HPV virus and that form is quite treatable, fortunately for me. The tongue cancer was also a squamous cell carcinoma but not of HPV origin.
Life on our lonely pale blue dot is strange. I’ll never get a full grasp of it. I’ll be on the top side of the grass for a while yet and until that changes, I’ll still be a student of the sciences and will continue to write about it.
As in the past, I will discuss some observations as a chemical scientist with cancer.
In 2013-4, I was treated for stage 4 squamous cell throat and separately, stage 4 prostate cancer and have been in remission since.
I picked up a new cancer as well as another precancer diagnosis a few weeks ago in late July, 2025. My very first colonoscopy (!!) identified several small precancerous polyps which were snipped out. The procedure was a breeze as was the much-derided colon-blow opening festivity. Propofol is amazing stuff.
Eleven days ago, I had my second partial glossectomy. The first in 2022 turned up a precancerous squamous cell lesion on the side of my tongue. The second, last week, removed a squamous cell tumor. A shallow, nickel-sized piece of tongue was removed along the middle-left edge. A skin graft from my arm was not performed, thankfully. Imagine having a hairy skin graft on your tongue!!
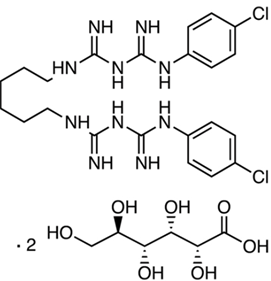
Prior to the surgery, I had to sanitize my arms, legs and torso with chlorhexidine (below as the gluconate), a common antiseptic. They even reamed out my nostrils with Povidone-Iodine. Incidentally Betadine is a trade name of Povidone-Iodine. First time for body-wide sanitization.
Graphic from chemical supplier TCI from Google images. This structure is the digluconate salt. Notice that the lower structure is a carboxylic acid and the chlorhexidine structure above is an is called a bibisquanide. Altogether there are 2 acid protons and 10 basic nitrogen atoms. The combination is actually an ammonium/iminium salt for water solubility.
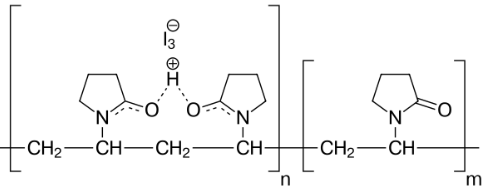
Povidone is the polymer poly(N-vinylpyrrolidone). It is used in many medicaments and is regarded as relatively safe. The chemical structure is shown below.
Image from Wikipedia. Povidone Iodine is a broad spectrum bactericide useful against bacteria, protozoans, fungi and viruses. It is prepared by combining PVP with hydrogen iodide and iodine. It slowly releases iodine in situ.
/*begin anecdote*/
Of interest to me is the use of N-vinylpyrrolidone. In a previous life I had prepared poly-NVP by solution polymerization on many occasions as a base for experimental liquid ink charge carriers in xerographic imaging. Very simple to make. The point was to replace existing liquid inks that used flammable hydrocarbon solvents. The startup who recruited my small startup went under because the solvent they were banking on didn’t dry fast enough for their economic model. The whole thing rode on the use of low viscosity 0.5 centistoke silicon fluids.
The business plan was to provide the photocopiers at low cost and then rack in the profits on consumables- a common strategy in the printing business. The founders were all retired from the giants of the photocopier industry. They knew all about the technology except for this seemingly small ink modification.
Alas, the drying rate was far too low and the image transfer was of persistent low quality. The elderly and retired engineer behind this invention fell over dead in the middle of it. He provided the patents but never actually built a prototype or even physically investigated the suitability of silicone fluids and ink composition. It was a big handwaving exercise that the founders bought hook, line and sinker. In the end, the sinker took them to the bottom still grasping for that golden ring they so desired.
/*end anecdote*/
The ever-popular opioid fentanyl was part of the basket of anesthetics used in the partial glossectomy procedure. A little mentioned side effect of fentanyl is extreme itchiness, particularly of the face. In post-op I had this in spades and it was very uncomfortable for several hours. My interest in the chemistry of fentanyl had never fully ballooned to include side effects.
The tumor board at the university hospital I go to voted that I should undergo exploratory surgery to examine the many nearby neck lymph nodes for evidence of spread. This would point to further treatment. My throat cancer was discovered when a swollen sentinel lymph node fused to my carotid artery and decorated my neckline.
I’ll admit that a salad of pessimism and resignation with breadsticks of nihilism has arrived at my table at life’s Olive Garden. Much depends on how the upcoming lymph node surgery will come out. We’ll have to wait and see.
Note: What follows are my observations and information from my oncologists and what is scraped off the interwebs. I try to seek information from either primary research literature, medical textbooks or from credible secondary sources. For treatment, I stick to a university medical institution and medical school faculty managing my treatment. I tend not to believe in dietary or nutraceutical approaches. It has been my observation that the origins of cancer are biochemically different from curative or preventative biochemistry. In other words, preventative measures by diet or supplements are mechanistically distinct from the treatment of cancer cells. Divine intervention is not testable, driven by faithful wishing and is supported only by anecdote. I believe that if something truly happens in the universe, it will have an observable mechanism and therefore be measurable.
Oh yes, if you’re squeamish with talking about your prostate because it’s part of your reproductive apparatus, get over it. Part of successfully living with cancer is being able to talk about and learning from it. I’d rather die at least knowing about it.
Because of modern medicine, my experience with both throat and prostate cancer has not been a rocket sled ride to the hereafter. It’s been said that some cancers can be thought of as a treatable, chronic condition and for me that has been true thus far. As luck would have it, my throat cancer was viral in origin and consequently highly treatable by IMRT irradiation and cisplatin. Since 2013 I have had yearly checkups that have all indicated no visible return of the cancer. Since I go to a university medical center, I have had medical students and various head and neck residents also peering down my throat from a camera threaded through my nose picturing my gullet in all of its pink glistening majesty.
The prostate story is a bit different. Before diagnosis the cells had already left the prostate (stage 4) and were judged to be Gleason 9 by histopathology. This was unfortunate. Outside of the prostate capsule they began to wander around through the lymphatic system, lodging in the lymph nodes. Since there was no unified target for surgery or concentrated radiation, The cutters were not called in. Elvis had left the building. After IMRT radiation of the prostate, seminal vesicles and suspected nearby lymph nodes along with 2 years of hormone ablation, my PSA returned to 0.01 ng/mL. Things had taken a turn for the better.
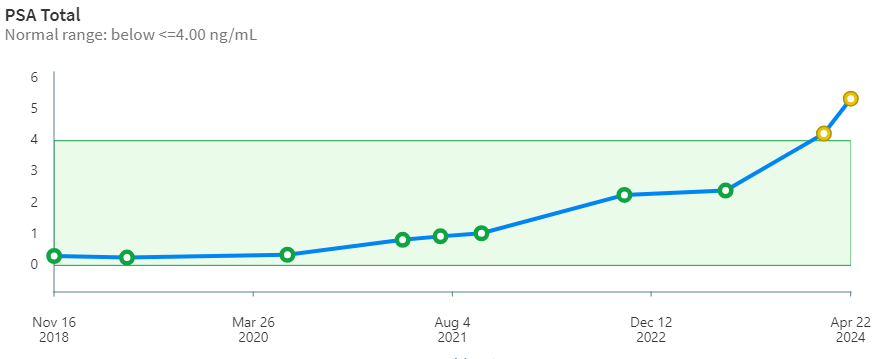
But, the other shoe had to drop eventually. After 9 years, my stage 4 prostate cancer has begun to ramp up steeply. The PSA curve over time (below) is looking more and more like a hockey stick. The borderline PSA value for treatment is 4.00 ng/mL. When it pops up over that value the oncologists begin to take notice. Whether this is based on some statistical mortality data or because of what insurance companies will likely cover is unclear to me. Importantly, PSA may also indicate non-cancerous conditions like prostatitis and benign prostatic hyperplasia. PSA is only an indicator and alone is not definitive. Biopsy is needed to verify and grade the tissue. Of this whole adventure, the biopsy was the worst of it for me. During the procedure, the urologist asked questions about my hobbies -his was carpentry- but I was too distracted to talk about airplanes.
Stage 4 is indicated by histology and backed up by the PET scan revealing radioactive (avid) spots outside of the prostate. Thankfully, this time around nothing was found in the head & neck, chest, prostate or bones. That was good news.
However, the PET/CT scan did show the presence of 5 or so avid lymph glands along the aorta from below the chest to above the prostate.
A proper prostate cancer diagnosis requires more than just a PSA value. An abnormal prostate is detected by digital examination by a urologist and the presence of cancer cells is confirmed by biopsy by a histologist.
My PSA curve.
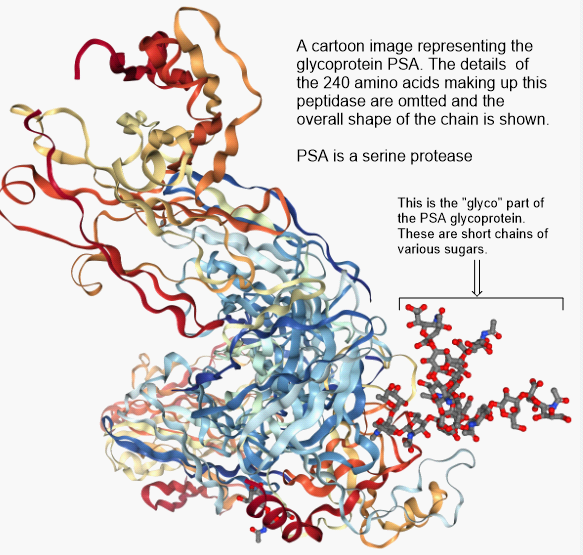
But, wait a minute. Exactly what is PSA and what does it do? According to Wikipedia, Prostate Specific Antigen (PSA) is a peptidase enzyme (a protein) secreted by the epithelial cells of the prostate gland. It’s immediate job is to liquify the semen in the seminal coagulum, allowing sperm to swim freely. It is also thought to be involved in dissolving cervical mucus, allowing sperm to enter the uterus. Amounts of PSA above a certain threshold are not normally found in the blood. Elevated PSA is associated with prostate cancer. It’s just a marker.
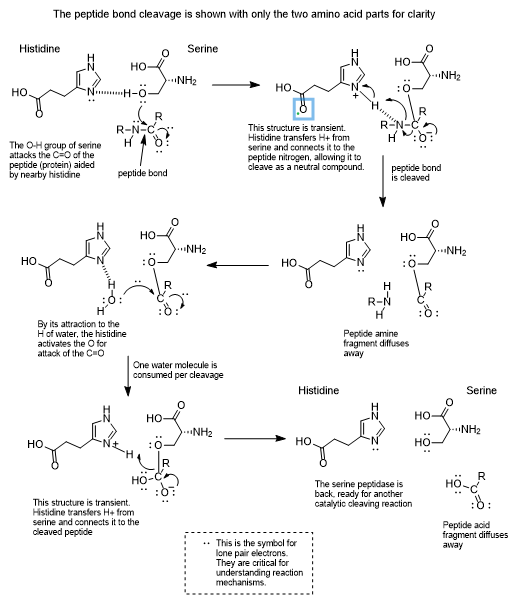
The glycoprotein PSA, prostate specific antigen. It is an enzyme of the serine protease variety. A protease will cleave peptide bonds in the amino acid backbone of a protein.
Serine protease enzymes like PSA have a serine amino acid in the active site of the enzyme which is capable of connecting temporarily with a carbonyl carbon of a (C=O) peptide bond. Since proteins are long chains of peptide bonds, cleaving a peptide bond snips the protein into smaller pieces.
Chemists are all about the mechanisms of chemical transformations and the following has been proposed for a serine protease.
All this said, it turns out that when castration resistance sets in, things begin take a turn for the worse. Prostate cancer cells begin to accumulate in the bone marrow, they begin to interact and develop into tumors that are essentially beyond the reach of treatment. The spine is a common place for them to go, but they can spread to other organs as well.
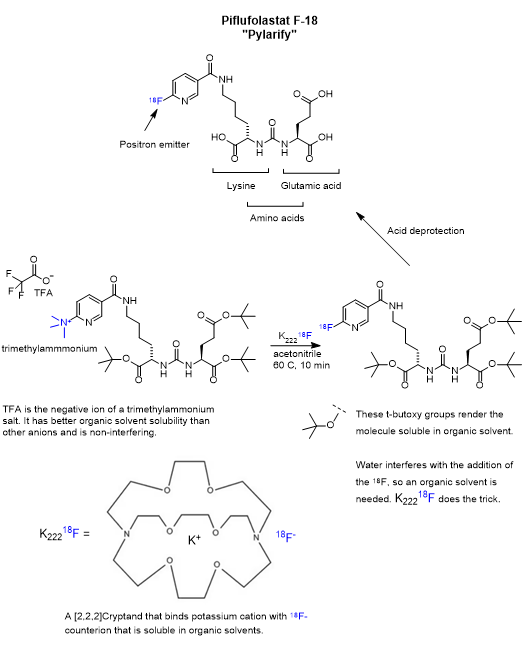
Of particular interest is the spread of prostate cancer to bone. Prostate cancer cells have an affinity for bone marrow tissue. In my case, the PET/CT scans gave no indication of being present in the head & neck, the chest or bones. That’s good news. In my first round of treatment, I was given 18F-Glucose diagnostic for the PET scan. This time I was given the more receptor-selective 18F PSMA diagnostic called Pylarify. While it is selective for a particular receptor on the cancer cell, it also shows up elsewhere in the body in the PET scan as a result of circulation and transport out of the system. Receptor-specific drugs will bind to the intended receptor, but only after they wander around and stumble into it. This is made less than random due to active transport or solubility partitioning. The effectiveness also benefits by resistance to metabolism and excretion.
Pylarify is a kind of pseudo-peptide containing two modified amino acids, lysine and glutamic acid, joined at the nitrogen atoms as a urea linkage. The key step is the nucleophilic aromatic substitution of trimethylammonium by 18F on the pyridine ring. The presence of abundant heteroatoms (nitrogen and oxygen) groups is not uncommon for pharmaceuticals and is absolutely ordinary for proteins. Heteroatoms serve as hydrogen bond donors and acceptors which is critical in biochemical transformations. A hydrogen bond donor can reversibly bind to a hydrogen bond acceptor and keep the molecules in close proximity long enough for a transformation as well as participate in it.
Sarah Piron, Jeroen Verhoeven, Christian Vanhove, Filip De Vos, Recent advancements in 18F-labeled PSMA targeting PET radiopharmaceuticals, Nuclear Medicine and Biology, Volumes 106–107, 2022, Pages 29-51, ISSN 0969-8051, https://doi.org/10.1016/j.nucmedbio.2021.12.005.
The story of PET, Positron Emission Tomography, has evolved over decades of advancement. To begin, tomography, detectors and computers had to be invented. Separately, positron emission as a medically viable radiation source had to be identified and validated. Positron decay occurs when a neutron deficient nucleus emits a positron and a neutrino to convert a proton to a neutron. This brings the p/n ratio to a more stable state.
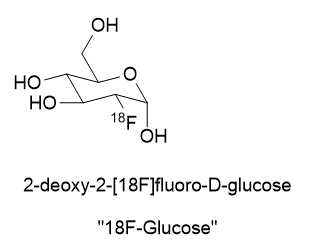
A substance for delivering a dose of isotope must be found. In the case of 18Fluorine, it is prepared as an inorganic salt like K18F or elaborated as an organic molecule like 2-deoxy-2-[18F]fluoro-D-glucose.
How did it come about that the 18Fluorine in the position where it is? I’ve not found mention of this in the literature so far. Looking through Chem Abstracts I have noticed there are numerous synthetic pathways leading to fluorine at that position. Could it have been placed there because research found that it was most biochemically similar to glucose? Or was it the more mundane reason that fluorination at position 2 gave the best yields and purity or was the cheapest and easiest to make?
18F has replaced the oxygen (OH) group at position 2 of glucose, thus the prefix “2-deoxy-2-[18F]fluoro-“
There are recent radioligand compounds that are used as PET (Positron Emission Tomography) diagnostic agents which selectively bind to the prostate specific membrane antigen receptor where they can undergo positron emission revealing the site of prostate cancer cells. 18F-glucose was first synthesized in 1967 in Czechoslovakia at Charles University by Dr. Josef Pacák and was first tried as a radiotracer by Abass Alavi in 1976 at the University of Pennsylvania on volunteers. PET scanning came along later. Cancer cells consume glucose a bit faster than normal cells so the 18F-glucose will tend to accumulate to a slightly greater extent and reveal their position by positron annihilation. This yields two 511 keV x-rays 180o apart and is identified by a ring coincidence detector. A single detection event is discarded.
Today, 18F-glucose is being superseded by many 18F PET preparations that are designed to interact with specific receptors. This interaction is called “conjugation”. In the case of Prostate Cancer there is PSMA, Prostate Specific Membrane Antigen, targeted by Pylarify (piflufolastat F 18) which is designed to bind with fatty acid binding protein 3 (FABP3). I just received a 6 millicurie (222,000 Becquerel) intravenous dose of this positron emitter just today for a PET/CT scan.
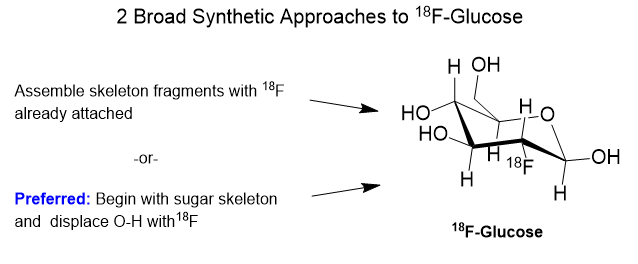
Synthetic Strategies Affording 18F-glucose
First, I have to say that the name 18F-glucose is a bit of a misnomer in that it is not glucose nor did it ever even start out as glucose. It is a 2-deoxy-2-18fluoro analog of D-glucose. It originates from D-Mannose whose OH groups were specially protected from side reaction by capping 4 of them with acetyl (Ac) groups and carrying away the hydrogens. The OH at position 2 of the D-Mannose precursor is converted to a triflate (OTf).
In chemical synthesis there is usually more than one possible strategy for getting to a target molecule. In the case of 18F-glucose, whatever pathway we choose must be rapid and efficient owing to the very short half-life of the 18F. The preparation must be done in as few half-lives as possible.
When it comes to a great many sugar derivatives, synthesizing them from scratch is just crazy. They are structurally and stereochemically complex. They have numerous hydroxyl groups in chemically different locations on the molecule and selective modification of one and not another can be quite involved. The world is awash in sugars (e.g., sucrose, starch and cellulose) from natural sources and many varieties are commercially available for developmental use. Better to adapt available sugars for modification than starting from earth, air, fire and water.
Source: Gaussling.
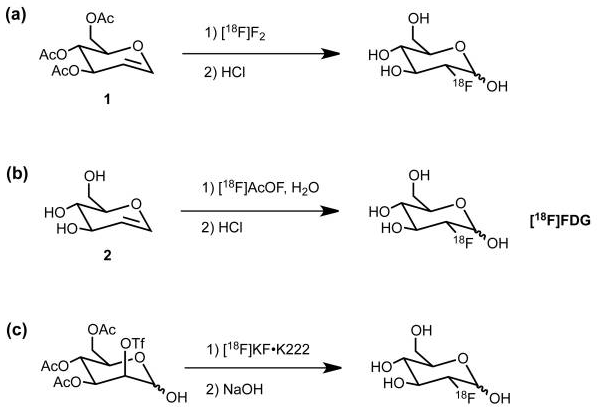
Getting 18F attached to a sugar can go along on one of two basic strategies- electrophilic addition of fluorine or nucleophilic addition. The first is called “electrophilic” addition where electrophile means “electron loving”. In electrophilic addition, the 18F reagent must be electron deficient requiring that the intended carbon skeleton is relatively electron rich. Electron rich means that there are oxygen or nitrogen atoms present with their lone-pair electrons, or pi-bonds present with their off-axis pi-electrons. Equations (a) and (b) below show two examples of electrophilic addition of 18F to a sugar analog.
The fluorinating reagents are (a) 18F enriched F2 and (b) acetyl hypofluorite, [18F]AcOF. Both fluorinating reagents feature fluorine atoms that are electron deficient and therefore electrophilic. Atomic and molecular fluorine are by nature quite electrophilic, but negatively charged fluoride is nucleophilic.
Source: Cole EL, Stewart MN, Littich R, Hoareau R, Scott PJ. Radiosyntheses using fluorine-18: the art and science of late stage fluorination. Curr Top Med Chem. 2014;14(7):875-900. doi: 10.2174/1568026614666140202205035. PMID: 24484425; PMCID: PMC4140448.
Nucleophilic addition of 18Fluoride is shown in reaction (c) wherein the OTf group is installed specifically to be displaced from the back side by 18F anion. A “nucleophile” is an attacking species that is able to bond directly with a carbon nucleus by virtue of having a lone pair of electrons available for bond making. A nucleophile is frequently negatively charged but can also be neutral in some cases.
The general strategy for the nucleophilic substitution synthesis of 18F-glucose is this: Protect all of the hydroxyl groups of D-Mannopyranose as an acetate except for one which serves as a “leaving group“. This leaving group is called a trifluoromethanesulfonate, or just “triflate“. This triflate is then displaced by 18Fluoride anion by an SN2 substitution. In plain English, 18Fluoride anion forms a C-F bond as the triflate anion is breaking its C-O bond in a process called nucleophilic substitution.
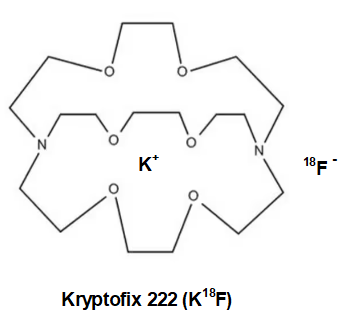
Oh, one more thing. The 18fluoride anion(-) must be made more reactive by keeping the inhibiting potassium cation (K+) in a “cage” so it can lose some of its electrostatic attraction to the negatively charged 18fluoride. Strong electrostatic attraction of K+ to 18F– will impede fluoride’s aptitude for triflate displacement. See below for Kryptofix 222. K+ wrapped in neutral Kryptofix 222 is called a “weakly coordinating ion”.
Ok, so there are some funny things you ought to know about this substitution business on a 6-member ring. Hydrogen atoms are not drawn because it is a pain. First, carbon always wants to have 4 bonds to it and oxygen just two bonds. Second, a 6-carbon ring with all single bonds can be twisted into several shapes or conformations. One of them is favored by virtue of having the least “strain” in it. That would be the “chair” conformation. It looks vaguely like a lawn chair.
Source: Gaussling. Shapes that cyclic, 6-carbon rings can take. In reality, the rings flip back and forth across the different conformations, but they tend to spend the most time in the lowest ring strain shape which is the chair.
Selective chemical synthesis happens only because some reaction pathways are fast while others are slow. Some possible reaction pathways are so slow that effectively they do not happen.
Making 18F
The 18F isotope does not exist in nature due to its 1.83 hour half-life. It decays by positron and neutrino emission to stable 18O. 18F must be prepared by slamming a suitable precursor nucleus with a nuclear particle like a proton or a deuteron with a cyclotron or linear accelerator. Yes, commercial cyclotrons are available for purchase.
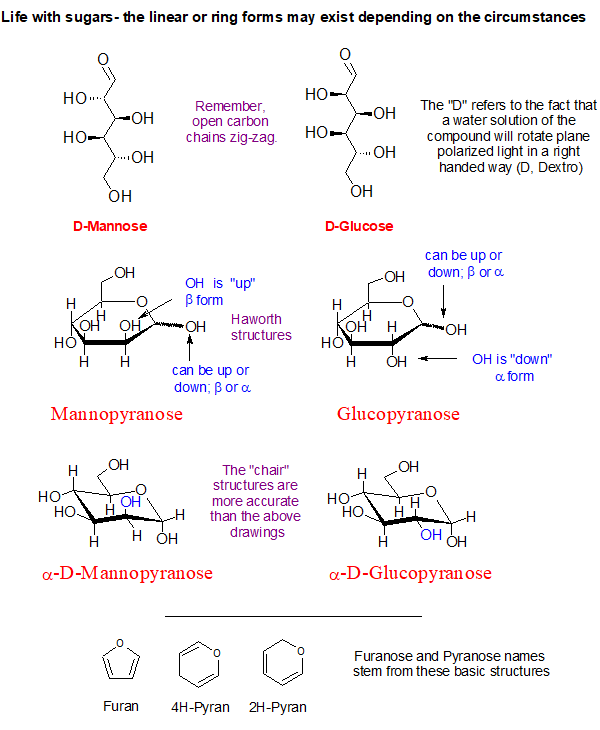
Some Sugar Facts
What helps when thinking about sugars is to detach them from the matter of sweetness. Sugars are far too diverse and important to get hung up on sweetness.
Look at the blue O-H groups on the α-D-Mannopyranose and compare it to the α-D-Glucopyranose shown above. See how they are hanging on the ring? One is directed up and the other is pointing outward and down a bit. This simple inversion in orientation produces the chemical difference between the two sugars making them distinctly different chemical substances.
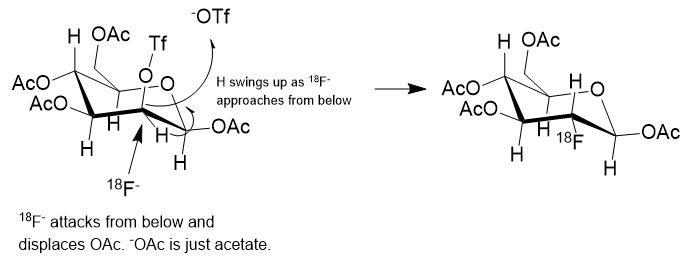
Source: Gaussling. How the 18-Fluorine gets attached to a sugar. D-Mannose is first derivatized by capping off 4 of the hydroxyl groups as acetates, OAc, and one as a triflate, OTf. 18-Fluoride backside attack will displace the triflate, –OTf. Of the –OTf and the –OAc, the –OTf is displaced much faster. The faster pathway dominates. The Ac groups are removed from their oxygens by base hydrolysis leaving OH groups on the ring behind. This results in the 18Fluorinated glucose.
In the reaction scheme above the 18F– is shown displacing the –OTf group from below, establishing a C-18F bond and causing the C-H to flip to the upper side like an inverting umbrella. The scheme is only partially correct. What isn’t shown is the positive counterion to the 18F– anion. The fluoride must be charge balanced by a positive ion which could be just a theoretical bare-naked ion or solvated potassium ion, K+.
In solution, ions or dipolar molecules interact with solvent molecules by Van der Waals forces or stronger dipolar influence. Going down the Group 1 elements on the periodic table from Lithium to Francium, all form 1+ cations, but also the radius of the ion increases. If you think of the ionic radius as being the distance from the nucleus to the distance that a solvent molecule can bump into, the Van der Waals radius, then as we drop down Group 1, a square picometer of “surface” of the ion carries less and less of the cationic charge at any given moment. This means that attractive or repulsive forces with that square picometer diminish as we go down the group, thus lowering the attractive forces. Very often potassium cation is acceptable, but it can be helped along.
While much of the time K+ is sufficiently non-interfering, but as happens occasionally the fluoride anion tends to bind to the potassium cation a bit too tightly. This can substantially slow the rate of transfer of 18F anion to the carbon of the sugar ring. To get around this, either the potassium must be replaced with another more charge diffuse cation like tetrabutylammonium+ or cesium+, the K+ can be “wrapped” in a protective organic “jacket or shield” that will prevent the K+ and the 18F– ions from getting too close to one another and bound too tightly. We would call the protected K+ a non-interfering or charge diffuse cation.
The cyclic amino polyether “ligand” that is used in this case in Kryptofix [2.2.2]. The single positive charge of the K+ is somewhat spread over the surface of the much larger Kryptofix [2.2.2]-potassium complex and diffuses the positive charge. This has the effect of “separating or loosening” an otherwise tight ion pair (K+F–) in solution. Once detached from potassium, the 18F– ion is able to react much faster to form the 18F-Glucose.
18F-Glucose must be synthesized in a radiopharmacy, also called a nuclear pharmacy, nearby the point of administration to the patient given its very short half-life. The 18F is produced in a commercially available cyclotron or linear accelerator either by proton bombardment of stable but scarce 18O enriched water or by deuteron bombardment of the stable isotope 20Neon.
18F-glucose is a sugar and undergoes metabolic trapping by phosphorylation with hexokinase inside the cell, giving it a phosphate group with a negative charge, inhibiting its transport to outside the cell. This allows the phosphorylated 18F-glucose to accumulate inside the cell, concentrating 18F to release more positron decays from the cell.
Prologue: What follows is a look at the use of 68Gallium as part of a positron emitting radioligand from an organometallic chemist’s point of view. I’m not from nuclear medicine nor am I a radiation oncologist.
It had to happen … the other shoe has dropped. My stage-4 prostate cancer has come charging back for round 2 after 9 years. Again, I’ve taken a personal interest in radiation oncology. Recently, my PSA shot up steeply through the 4.0 ng/dL threshold triggering an appointment with my radiation oncologist who has ordered a PET/CT scan. Back in 2015 I finished 18 months of hormone ablation (chemical castration) and got the PSA from 29 down to 0.01 with Lupron injections and earlier, a large cumulative dose of x-radiation in the lower abdomen. I have to say that while I experienced no discomfort at all in this round of treatment, I did lose body hair and muscle mass.
PET/CT scanning is an important tool in locating prostate cancer cells. Riding the platform in and out of the scanner is expensive but important. Unfortunately for me, the CT contrast agent is a potent emetic so the scanner becomes an expensive vomitorium ride.
The story of PET, Positron Emission Tomography, has evolved over decades of advancement. To begin, tomography, detectors and computers had to be invented. Separately, positron emission as a medically viable radiation source had to be identified and validated. A substrate for selective delivery of the isotope must be found. In the case of 18Fluorine, it is available as an organofluorine molecule like 18F-Glucose. It turns out that the 18F-Glucose concentrates in clinically useful places and K18F does not.
Positron Emitters
Atomic nuclei that are deficient in neutrons can have an instability leading to emission of a positron (anti-electron with a + charge), also called a β+ decay, which lessens the neutron deficiency by ejecting a positive charge from the nucleus. When a positron is ejected from the nucleus it finds itself immediately swarmed by the electron clouds of surrounding atoms and molecules and doesn’t travel very far. When a positron encounters a negatron (regular electron, β−), they annihilate one another and emit two gamma photons of 511 keV energy at 180 degrees apart. This is a mass to energy conversion. Loss of one positive charge from the nucleus gives rise to a transmutation of the atom causing a one-unit drop in atomic number, that is it goes from n+ to (n – 1)+, but retains most of its atomic weight. In this case, 6831Gallium undergoes positron decay to 6830Zinc.
Positron emitters include 11Carbon (T1⁄2 = 20.4 min), 13nitrogen (T1⁄2 = 10 min), 15oxygen (T1⁄2 = 2 min), 18fluorine (T1⁄2 = 110 min), 64copper, 68gallium, 78bromine, 82rubidium, 86yttrium, 89zirconium, 22sodium, 26aluminium, 40potassium, 83strontium, and 124iodine. This a list given by Wikipedia, but there are many more in more comprehensive tables.
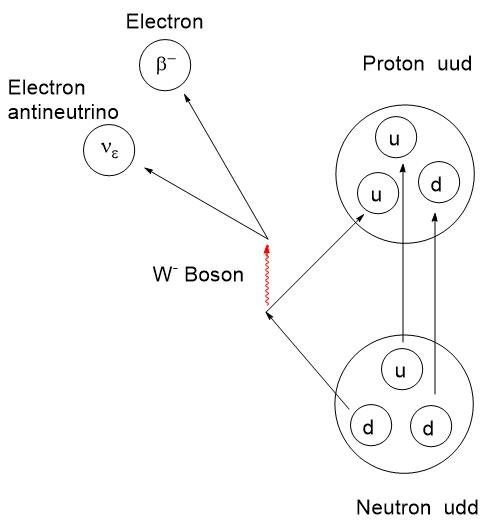
The actual mechanism of β-type emission requires a venture into fundamental particles called quarks. Protons and neutrons are composite particles called hadrons, not fundamental particles. Protons and neutrons are each comprised of 3 quarks, but with a different combination of “up and down flavors” where flavor refers to the species of quark. There are 6 flavors of quarks: up, down, charm, strange, top, and bottom. Interconversion between protons and neutrons can occur if one of the 3 top or bottom quarks changes flavor. By all means, if this interests you, take a dive into it. I shall stop here.
Beta emission diagram at quark level.
Positron emitters tend to have a short radioactive half-life as well as a limited chemical half-life in the body before they are cleared out through the kidneys or other routes. Ideally, the goal is to deliver a high radiation dose selectively to a target tissue as fast as is safe then disappear. Prolonged irradiation to surrounding tissue is undesirable. The optimal radiopharmaceutical will be highly target selective and have a short half-life. A selective radiopharmaceutical is one that will accumulate in a desired cell type or organ. Accumulation can be aided through simple solubility, the ability to undergo transport through a cell wall, affinity to a specific receptor and the ability to function fast enough to resist the various clearance mechanisms.
A short half-life means that the radioactivity per gram of radioisotope, specific activity in Becquerels per gram, will be at its maximum after activation. Though the radioactivity may be intense, the radiation dose can be controlled by the amount of mass administered. With radioisotopes, there are two kinds of purity to consider: Chemical purity referring to the atoms and molecules present; Radiological purity referring to the presence or absence of other radioactive isotopes. To provide maximum safety and effectiveness, the specific radioisotope with the desired decay mode should be the only source present. If your desired source is an alpha emitter, you don’t need spurious quantities of a gamma emitter present because of inadequate purification.
Economical methods of preparing positron emitters had to be addressed. To fully exploit PET for any given situation, tissue selectivity of radioligands had to be determined and selective positron radiopharmaceuticals developed. Due to the short half-life of these radioisotopes, rapid and safe methodologies to produce them by efficient nuclear transformations, isotope isolation followed by chemical synthesis had to be developed. It is important that isotope generation, isolation and attachment to a ligand be done nearby the hospital for the proper activity to reach the patient.
Positron emitter production involves a nuclear reactor for neutron activation or a cyclotron accelerating protons or deuterons in the preparation. Because both of these sources are highly destructive to organic molecules, an inorganic radioisotope is produced separately and chemically modified to produce an inorganic species that can be chelated or otherwise attached to a radiopharmaceutical. This technique evolved from simple radiography in the 1930’s to a large array of techniques and applications today. The reader is invited to take a dive into this topic.
Since my cancer experience began, a few new radiotherapies and imaging agents have landed in oncology space for prostate cancer. Recently I posted on Pluvicto PSMA (Prostate Specific Membrane Antigen) which was before I knew about my current prostate situation. PSMA is a transmembrane protein present in prostatic cells. Pluvicto uses a chelated177Lutetium beta emitter as the destructive warhead and a peptidomimetic fragment for binding to the PSMA receptor.
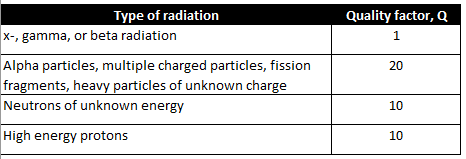
A Brief Interlude into Quality Factor
It should be noted that the various forms of particle (alpha, beta, or neutron) or electromagnetic radiation (x-ray or gamma) have differing abilities to penetrate and cause ionization of within matter. There is a factor for this which is used to refine dosage calculations. It is called the Quality factor, Q.
The destructive effects of radiation stem from its ability to ionize matter along its path. Ionization is a disruptive effect that may result in fragmentation of molecules or crystal lattices into reactive positive or negative ions. Single electron radical species may be formed as well. It is possible for some fraction of the disrupted molecules to recombine if the fragments haven’t already diffused away or gone on to further transformations.
The deleterious effects of radiation on living tissue stems from the amount of disruptive energy transferred to tissues along the path of each particle. Charged particles like electrons, protons and alpha particles tend to dump their energy into matter rapidly and along a short path making them less penetrating than neutrons or electromagnetic rays in general.
Quality factor, Q, is a dimensionless coefficient that is multiplied by an absorbed dose to give a more realistic estimation of radiation energy absorption. Interestingly, the Q for neutrons varies with energy and rises to a maximum around 0.5 to 1 MeV of energy and falls off at higher energies.
The larger the Q factor, the larger the corrected radiation effect. X-, gamma, and beta radiation have a Q factor lower than the others by a factor of 10 to 20. The x- and gamma rays will tend to pass through matter leaving a small amount of their energy to disruption. In radiation therapy this is compensated for by just increasing the fluence or the exposure time.
For clarity, x-rays are generated from the electron cloud around an atom via electron transitions. For instance, if an electron is dislodged from an inner, low energy orbital, another electron can occupy that vacancy by the emission of an x-ray. Gamma rays originate from nuclear energy transitions. Often a nuclear decay might result in a new nucleus that is not at its ground state and would be categorized as metastable. This metastable state, which has its own half-life, can collapse to its ground state by the emission of a gamma ray matching the loss of energy by the nucleus.
Neutrons
Free neutrons are special. They undergo beta decay with a short half-life outside the nucleus having t1/2 = ~ 10-15 minutes, depending on the information source. Not having a charge, they tend to be more penetrating than other particles. However, effective shielding can be had with a hydrocarbon like paraffin or water by virtue of the high concentration of hydrogen nuclei present in these substances. Neutrons are not affected by charge repulsion from an atomic nucleus and therefore can collide and interact with the hydrogen nucleus (a proton). They can scatter from hydrogen nuclei, leaving behind some of their kinetic energy with each collision (see “Neutron Lethargy“). This scattering is the basis for using water to moderate the neutrons in a nuclear reactor. Neutrons are cooled by repeated collisions with hydrogens in water to the point where their kinetic energy of 0.025 eV, which from the Maxwell-Boltzmann distribution corresponds to a temperature of 17 oC, thus the term “thermal neutrons“.
Many elements absorb neutrons, increasing the atomic weight and very often altering the stability of the nucleus leading to a radioactive decay cascade. This is what is happening in neutron activation. In the case of water, the ability of free neutrons to collide with hydrogen nuclei allows them to dislodge hydrogen ions or free radicals from organic and biomolecules resulting in ionization and makes them quite hazardous to living things.
Radioligands
Drugs like Pluvicto are referred to as a radioligand. There is a radioisotope connected to an organic “ligand” for selective binding to a specific protein receptor. A radioligand is injected and diffuses its way a particular receptor where it binds. As it turns out, due to the gamma radiation also emitted by 177Lu, Pluvicto is a radioligand that can also be located in the body by the gamma radiation it emits. In general, a radioligand can be used for two endpoints: To find and signal the location of a particular cell type; and to find and vigorously irradiate a particular cell type.
There are recent radioligand compounds that are used as PET (Positron Emission Tomography) diagnostic agents which selectively bind to the PSMA receptor where they can undergo positron emission revealing the site of prostate cancer cells by tomography. 18F-glucose was first synthesized in 1967 in Czechoslovakia at Charles University by Dr. Josef Pacák and was first tested as a radiotracer by Abass Alavi in 1976 at the University of Pennsylvania on volunteers. Positron tomography came along later. Cancer cells consume glucose faster than normal cells so the 18F will tend to accumulate to a slightly greater extent and reveal their position by positron annihilation. The two 511 keV x-rays simultaneously detected at 180o apart are identified by a ring coincidence detector. A single detection event is discarded.
Dr. Abass Alavi, University of Pennsylvania. First use of 18F-Glucose on humans.
Dr. Josef Pacák (1927-2010), of Charles University in Czechoslovakia. First to prepare 18F-Glucose.
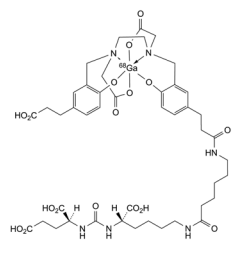
A radioligand that received FDA approval the same day as Pluvicto was Locametz or Gallium (68Ga) gozetotide. This gallium radioligand targets PSMA as does Pluvicto but is only a PET diagnostic agent.
Locametz or Gallium (68Ga) gozetotide. Source: Pharmeuropa.
Locametz has 4 carboxylic acid groups, a urea group and two amide groups aiding water solubility and numerous sites for hydrogen bonding of this radioligand to the receptor. The organic portion of the Locametz is called gozetotide, named “acyclic radiometal chelator N,N’-bis [2-hydroxy-5-(carboxyethyl)-benzyl] ethylenediamine-N,N’-diacetic acid (HBED-CC).” The 68Ga (3+) cation is shown within an octahedral complex with a single hexadentate ligand wrapping around it. The short 68 minute half-life of 68Ga requires that a nuclear pharmacy be nearby to prepare it. The short half-life of 68Ga or other positron emitters as well as the possibility of destructive radiolysis to the ligand prevents preparing a large batch and stocking it. Locametz must be synthesized and transported prior to use. This rules out remote or rural hospitals.
Nuclear Chemistry
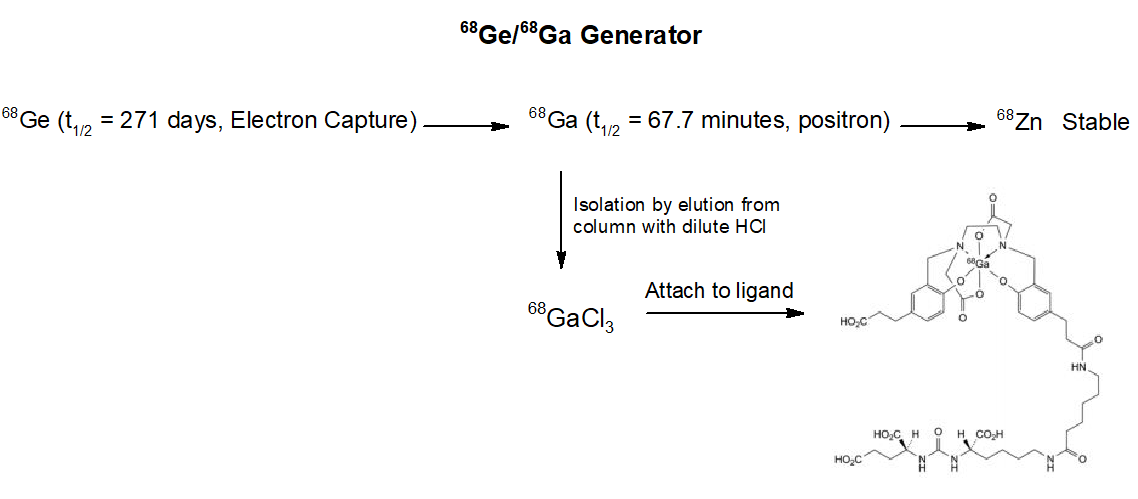
So, where does one obtain 68Gallium? Well, there are several methods out there. 68Ge/68Ga generators are produced commercially. One company is GeGantTM who offers 1-4 GBq of 68Ga. (Note: 1 GBq is 1,000,000,000 disintegrations per second).
Diagram courtesy of Gaussling.
From the scheme above we see the workings of a 68Ga generator. The ligand attachment is performed exterior to the generator. Atomic nuclei that are neutron deficient like 68Germanium can transform a proton to a neutron. There are two ways this can happen. In Electron Capture (EC) an inner “s” electron can be absorbed by a proton converting it to a neutron and emitting a neutrino by the weak nuclear force. This lowers the atomic number by 1, in this case 6832Germanium becomes 6831Gallium. The other mechanism is for the nucleus to emit a positron (anti-electron) and eject 1 positive charge as a positron (and an antineutrino) from the nucleus, resulting in a new neutron. The atomic weight remains constant, but the atomic number drops by one. If available energy in the nucleus is less than about 1 MeV, an electron capture is more favorable than positron emission.
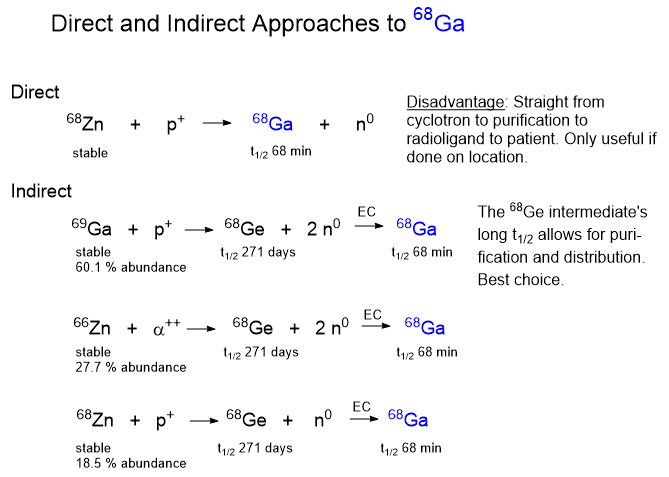
Once you know about the 68Ge electron capture reaction leading to the 68Ga isotope you have to ask, where does the 68Germanium come from? There are a few different ways to make and concentrate 68Ge and the method you use depends on the equipment available to you. One way is to accelerate protons to a high energy in a cyclotron and slam them into atoms heavier than germanium, such as rubidium or molybdenum. The collision with break the target nuclei into pieces by a process called “spallation“.
Diagram courtesy of Gaussling.
Cyclotrons
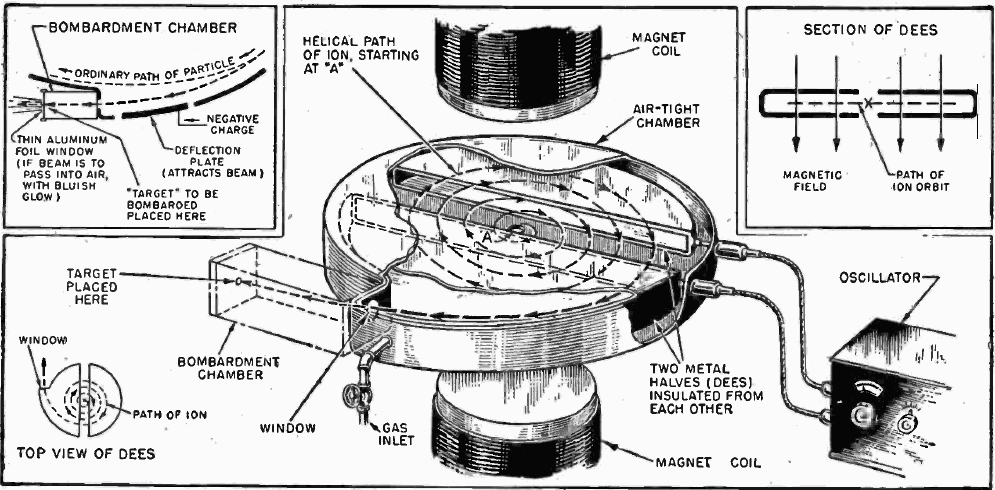
The first cyclotron was independently invented by Ernest Lawrence 1929-1930 at UC Berkeley. It was the first cyclic particle accelerator built. The idea of the cyclic accelerator was first conceived by German physicist Max Steenbeck in 1927. In 1928-1929 Hungarian physicist Leo Szilard filed patent applications for a linear accelerator, cyclotron, and the betatron for accelerating electrons. Unfortunately for both Steenbeck and Szilard, their ideas were never published or patented so word of the ideas were never made public.
Where does one go to get a cyclotron? One company is Best Cyclotron Systems. If you are not sure of how a cyclotron works, check out the image below from Wikipedia. Note: A cyclotron can only accelerate charged particles like protons, electrons, deuterons and alpha particles which are introduced into the middle of the machine. A key component is the “D” or Dee, so-called because of their D-shape. The cyclotron has two hollow, coplanar Dees which are each connected to a high voltage radiofrequency generator. The Dees are open chamber-shaped electrodes that alternately cycle through positive and negative high voltage attracting and repelling charged particles under the influence of a powerful magnet. Because charged particles change their trajectory under the influence of a magnetic field, the particles follow a curved path of increasing diameter, accelerating until they exit the Dees and careen into the target.
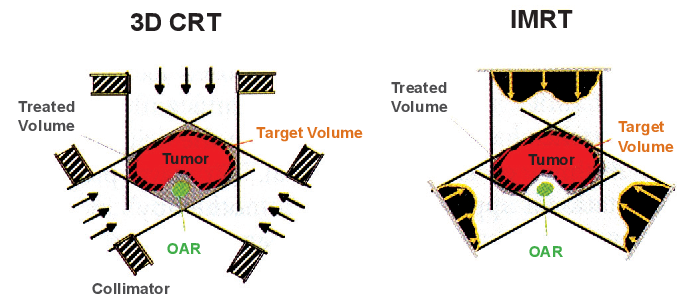
It has been right at 10 1/2 years since I was treated for squamous cell throat cancer. This virally induced cancer is quite treatable with a high success rate. The treatment was simultaneous radiation and cisplatin. The x-radiation dose was 68 Gray in daily 2 Gray doses with 6 cisplatin infusions. The radiotherapy machine was an Intensity Modulated Radiation Therapy (IMRT). The source rotates around the stationary patient varying the beam size and intensity as it goes. The idea is to put the energy into the tumor and spare healthy tissue to the greatest extent possible. The neck is a very crowded place with many kinds of tissues you don’t want to zap too much.
Illustration showing variable intensity beam shaping from the IMRT on the right. Source: Semantic Scholar.
It took about 1 week for the radiation effects to show up. It began with a sore throat which quickly led to a stomach feeding tube. They snake a pointy-ended tube down your throat and poke it out of your belly. I had it in for about 6 weeks. I jammed my liquid food in with a 60 mL syringe.
Besides the considerable discomfort from the radiation, long term side effects were not terrible. My thyroid took a big hit as did my salivary glands and taste buds. Ten years of dry mouth has led to the loss of some teeth. And, there was difficulty in swallowing initially. This problem unexpectedly returned during my recent bout of pneumonia.
The cisplatin was given in 6 doses. The nursing staff in the infusion suite don considerable PPE while handling chemotherapeutic drugs due to the toxicity hazard. I had no noticeable symptoms from this treatment. But while in the infusion suite, I could hear numerous female patients who were groaning in misery and vomiting from their meds. It was heart wrenching.
Nine years ago I wrapped up radiation for my stage 4 prostate cancer. Though the dose was lower at 38 Gray, there were no real negative effects as with the throat radiation. This was followed by 2 years of chemical castration with Lupron. It is also called hormone ablation. Lupron interferes with the production of testosterone. It does not, however prevent the adrenal glands from producing it, but this is a minor source. The first effective treatment for prostate cancer was surgical castration done to halt testosterone production. This hormone accelerates the growth and spread of the cancer. These guys who take testosterone for body building have no idea about the other thing the hormone can do. Just my opinion.
Hormone ablation eventually becomes ineffective because over time the prostate cancer cells respond by increasing the number of androgen receptor proteins on the cell walls. After hormone ablation fails, more severe treatments are put into use.
My outlook is this- The throat cancer is unlikely to return, but the prostate cancer will eventually take me out. I’ve had plenty of time to ponder death since the cancer diagnoses. I’d much prefer to have a quick, fatal heart attack than a slow, wasting death from cancer. I jokingly mentioned this to my cardiologist. He replied that the heart attack might not kill me. Buzzkill.
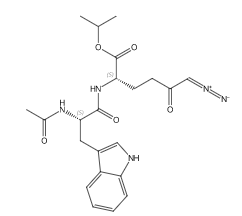
An anti-cancer prodrug called Sirpiglenastat (DRP-104) is in the news. The mode of action is in part the antagonism of glutamine metabolism. In a paper published in Molecular Cancer Therapeutics (DOI:10.1158/1535-7163.mct-22-0282), the authors describe the broader actions of the prodrug-
“DRP-104 demonstrated significant antitumor activity as a monotherapy, which was further enhanced in combination with checkpoint blockade therapies, leading to improved survival and long-term durable cures. In summary, DRP-104 broadly remodels the tumor microenvironment by inducing extensive tumor metabolism effects and enhancing the infiltration and function of multiple immune cells distinct from those obtained by checkpoint inhibitor therapy.”
I’m an organikker but not a medicinal chemist. What struck me as interesting is the presence of a diazocarbonyl group on the molecule. This functional group isn’t often found on drug molecules. In the larger scheme of things, there is nothing extraordinary about synthetic chemistry with diazocarbonyl compounds as intermediates for drug molecules, but diazo groups on drugs or natural products is quite a bit less common.
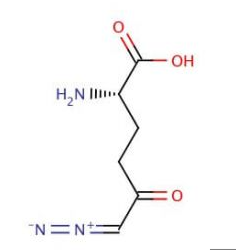
“Broad glutamine antagonism with sirpiglenastat (DRP-104). Sirpiglenastat (DRP-104) is a tumor-targeted prodrug of the glutamine antagonist 6-diazo-5-oxo-l-norleucine (DON), which was identified in the 1950s as a potent anticancer agent (79). DON is a mechanism-based, irreversible inhibitor of all glutamine-utilizing enzymes (80), and thus broadly inhibits metabolic pathways that require glutamine as a nutrient source. The main impediment in the clinical development of DON has been its dose-limiting toxicities to normal tissues (81), especially the gastrointestinal tract, which is highly glutamine dependent (82). By utilizing promoieties that are preferentially cleaved by tumor-enriched enzymes (83), sirpiglenastat is able to deliver DON preferentially to the tumor, increasing its therapeutic index.”
6-diazo-5-oxo-l-norleucine (DON)
The glutamine antagonist 6-diazo-5-oxo-l-norleucine (DON) mentioned above was isolated from a streptomyces culture found in Peruvian soil. The Wikipedia article mentioned that DON works by alkylation at the active site of the glutamine utilizing enzyme (I’m not happy with this source, but a Google search for a primary reference was not successful). Due to systemic toxicity, DON is not currently in development.
Note: This was written a year ago. The throat and prostate cancers are currently in remission and I have had time to enjoy the new stents in my right coronary artery. In the last few years I’ve been sonicated, dissected, radiated, biopsied, chemically castrated, spiked with positron emitters, poisoned with platinum, and stented. Yes boys and girls, what a delightful time it has been.
It doesn’t take long in one’s treatment regimen to see that a large industry consisting of diverse technologies has grown around cancer. As one is lead through the maze of corridors and treatment plans, it becomes apparent that the treatment centers are backed by some serious industrial might. As I walk into the cancer center my blood pressure is taken by an automated device, a digital scale takes my weight, and a small device with a light source in it takes my blood oxygen. The staff unlocks the terminal with a fingerprint reader and enters the data into my patient file. The doctor and a dapper young resident soon arrive and consult the terminal. Blood tests are short turnaround and performed on site. The onco-doc and the resident look at the results and divine some kind of conclusion from the numbers.
In nuclear medicine, a local 18F provider produces F18-labeled drugs for daily delivery to the rad labs in small leaden containers. Shortly before delivery a radiochemist quickly isolates the 18F (KF?) and prepares the 18F-glucose that the patient will receive as an injectable from a shielded syringe.
After a bit of resting time to allow the radio-sugar to circulate, the radioactive patient is placed on a motor-driven table that slides into an integrated CT-PET scanner for a bit of tomographic wizardry. A 3D x-ray map of the body is reconstructed from the CT beam data. As soon as the x-ray data is captured, the adjoining PET scanner is switched on and the patient is moved into the sensing zone of the device where gamma rays emissions reveal their location in three dimensions. After the data is collected, it is superimposed on the X-ray CT image to show anatomical locations that indicate an excess accumulation of the glucose. Cancer cells, being immortal and capable of mobility, can reproduce at a higher rate that normal cells. This leads to increased glucose uptake and, accordingly, a greater concentration of radiolabeled deoxyglucose in the cancer cells. A greater concentration of 18F-labeled glucose betrays the location of concentrated cells as they light up in the gamma spectrum.
The pharmaceuticals for chemotherapy are often quite toxic so the nurse who administers the drug is required to don PPE for preparation and administration of the dose. Specialized furniture is provided for the comfort of the patient and family. In the infusion suite of UC Hospital patients lie on recliners within a walled space with a view of the outdoors. Many patients watch familiar television programs as poison drips slowly into their veins. Some patients get sick relatively soon and succumb to fits of vomiting. Others are so strung out from the treatments that they lay there impassively. Worried family and friends strive to manage their own fears while trying to be attentive and positive.
Everywhere in the hospital disposable implements are used. The amount of sterile consumables used by a busy hospital is substantial. Sterile wrappers, clam shell packaging, syringes, IV bags, gauze, tubing, etc. I doubt that the shadows of medical and nursing students ever darken an autoclave anymore.
The breadth of technology and applied science in a hospital is staggering. Microprocessors monitor a wide variety of sensors that then produce digitalized output to either a dedicated screen display or to a nursing station.
The whole system at the hospital is devised to use every available minute of the physicians time. Receptionists verify the patient’s identity and assure the computer that the insurance information is in place. Patients are lined up for entry to the examination rooms.
At a university hospital, physician/professors on duty may have students and residents in tow to observe the great variety of disease states covering a wide range of illnesses. In a recent visit to my head and neck onco-doc, the three polite medical students took turns noodling the scope in my throat to get a thorough look-see. I had all I could do avoid laughing while the students took turns carefully manipulating the slender optical fiber device as it twisted about up through my nasal spaces and emerged below the uvula. The monitor displayed in sharp definition the glistening pinkish tissues in the treatment zone. As before treatment the primary tumor was not visible to the eye.
The industrial cancer business is vast, staffed by highly educated people, data driven and supported by a web of supply chain industries. The extent of the integration of data management is apparent as soon as you check in. Before the appointment is granted your identity and insurance status are verified by the accounting system and copayment is taken. An assistant guides you into a room where digital equipment takes your vital signs and the results are loaded into your patient record on the spot. You wander into another room and the nurse records the purpose of the visit and takes note of your vital signs and history. Soon the doc ambles in, logs into the data system and reviews the information. The appointment begins in earnest.
Those of us in our late 50’s have lived long enough to witness the gradual takeover of electronic and data technology in every aspect of our lives. In the early 1960’s, most of our lives were entirely analog. Television, radio, film, music, automobiles, and general business activities were largely conducted with technology that was fundamentally analog in nature. That is, energy was manipulated or work done via frequency or intensity modulation of electrical properties or by machinery powered by distant turbines. Devices driven by binary math and Boolean logic were around obviously but were only just beginning to enter the consciousness of common folk.
The point is that computer technology has, over a short interval, applied novel decision making or influences on the most intimate elements of our individual existence: The conduct of our wellbeing and how we process the never-ending stream of bewildering sensory input into our consciousness. Applied to the present discussion, health care providers and patients today face a torrent of data in the form of images and measurements that must be wrought into some kind of picture that people can comprehend and use to make plans. Inevitably there are data that, while accurate, are irrelevant to a given issue. And inevitably there are still questions that cannot be answered honestly owing to a fundamental lack of understanding.
For the patient there is a bewildering stream of science-based information and not so sciency information. There is a tendency in people to pay attention to optimistic product testimonials by other afflicted individuals. Magazines and cable television telegraph anecdotal sales pitches at people desperately seeking relief and even a cure. Many people feel the allure of anti-establishment messages promoting dietary plans. There is much talk of anti-oxidant, cleansing and herbal approaches to the treatment of disease states. The fact is, substances which might very well have cancer-preventative properties may be quite useless in the treatment of cancer.