First let me say that I have never been a smoker, drug user or sun bather. As a chemist I have always been cautious about chemical exposure. I have numerous cancers now with the two serious ones in remission. The new ones- who knows.
I use a university hospital and have been visited by flocks of med students looking at me in wonder, sometimes looking down my throat. I get a kick out of it. I always try to joke with them. All cancer diagnoses go before a faculty tumor board for collective assessment. That in particular drew me to this hospital.
My experience with numerous radiation, medical, ENT, and head & neck oncologists is that they absolutely do not want to discuss end of life issues. Maybe that is because I’m not near the end yet, though. But more likely they have production quotas and need to stick to the timeline. My head and neck oncologist did say that they were trying to keep me above the grass, though. That was cheerful.
Since July 22 of this year, I’ve had a partial glossectomy to remove a tumor resulting in a nickel-sized piece of the left edge of my tongue being removed, my first colonoscopy, a neck dissection looking for more cancer, and tomorrow is a root canal. Sonofabitch!
The glossectomy resulted in giving me slurred speech and then the neck dissection made it much worse with the added joy of serious swallowing difficulty. Liquids must be thickened with carrageenan gum to mostly avoid inhalation of food and drink. I’ve already been hospitalized with pneumonia resulting from inhaled food.
My 68th birthday was last week and while I received my well wishes, not a single person was moved to suggest a gerontologist, elder care facility or even as little as when the word “elderly” is used. I’m left up in the air …
It never occurred to me earlier in life that a piece of my tongue could be sliced out. What part of your body is more intimate in your daily consciousness than your mouth? I’ve had surgeons say “give me control of your tongue”. A fella doesn’t hear that very often.
The colonoscopy revealed 2 polyps suspected of being cancerous. So, to tally up the score, I have stage 4 prostate cancer, stage 4 throat cancer, tongue cancer, basil cell skin cancer, and possible colon cancer. Jesus H. Christ!! What next?.
The radiation of my throat resulted in the loss of about 1/2 of my salivary glands and taste buds. I’ve had dry mouth since radiation treatment in 2013, resulting in the loss of numerous teeth.
I was given radiation treatment of my prostate in 2014 and again last summer when the PSA score breached the 4.0 level. Since the 2014 treatment the thinking has changed on radiation dosage. Previously I was given about 1.8 Gray per dose. This time it was 5.0 Gray per dose over fewer doses. The thinking is that it is better to try to break the cancer cell DNA in 2 places at once rather than in just one place. In two rounds of x-radiation treatment of my prostate, I have experienced no pain or discomfort. I’ve had two rounds of 18F-Glucose injections for PET/CT scans.
The throat radiation was a different story. It gave me the world’s worst sore throat. I was fed through a stomach tube and was on opioids for an extended period. Let me say that I detest opioids and the constipation they bring. How do opioid addicts deal with this??
The throat cancer was from the HPV virus and that form is quite treatable, fortunately for me. The tongue cancer was also a squamous cell carcinoma but not of HPV origin.
Life on our lonely pale blue dot is strange. I’ll never get a full grasp of it. I’ll be on the top side of the grass for a while yet and until that changes, I’ll still be a student of the sciences and will continue to write about it.
Note: What follows are my observations and information from my oncologists and what is scraped off the interwebs. I try to seek information from either primary research literature, medical textbooks or from credible secondary sources. For treatment, I stick to a university medical institution and medical school faculty managing my treatment. I tend not to believe in dietary or nutraceutical approaches. It has been my observation that the origins of cancer are biochemically different from curative or preventative biochemistry. In other words, preventative measures by diet or supplements are mechanistically distinct from the treatment of cancer cells. Divine intervention is not testable, driven by faithful wishing and is supported only by anecdote. I believe that if something truly happens in the universe, it will have an observable mechanism and therefore be measurable.
Oh yes, if you’re squeamish with talking about your prostate because it’s part of your reproductive apparatus, get over it. Part of successfully living with cancer is being able to talk about and learning from it. I’d rather die at least knowing about it.
Because of modern medicine, my experience with both throat and prostate cancer has not been a rocket sled ride to the hereafter. It’s been said that some cancers can be thought of as a treatable, chronic condition and for me that has been true thus far. As luck would have it, my throat cancer was viral in origin and consequently highly treatable by IMRT irradiation and cisplatin. Since 2013 I have had yearly checkups that have all indicated no visible return of the cancer. Since I go to a university medical center, I have had medical students and various head and neck residents also peering down my throat from a camera threaded through my nose picturing my gullet in all of its pink glistening majesty.
The prostate story is a bit different. Before diagnosis the cells had already left the prostate (stage 4) and were judged to be Gleason 9 by histopathology. This was unfortunate. Outside of the prostate capsule they began to wander around through the lymphatic system, lodging in the lymph nodes. Since there was no unified target for surgery or concentrated radiation, The cutters were not called in. Elvis had left the building. After IMRT radiation of the prostate, seminal vesicles and suspected nearby lymph nodes along with 2 years of hormone ablation, my PSA returned to 0.01 ng/mL. Things had taken a turn for the better.
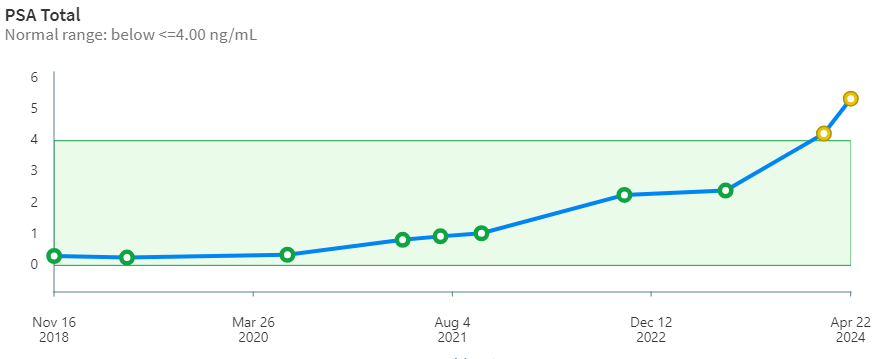
But, the other shoe had to drop eventually. After 9 years, my stage 4 prostate cancer has begun to ramp up steeply. The PSA curve over time (below) is looking more and more like a hockey stick. The borderline PSA value for treatment is 4.00 ng/mL. When it pops up over that value the oncologists begin to take notice. Whether this is based on some statistical mortality data or because of what insurance companies will likely cover is unclear to me. Importantly, PSA may also indicate non-cancerous conditions like prostatitis and benign prostatic hyperplasia. PSA is only an indicator and alone is not definitive. Biopsy is needed to verify and grade the tissue. Of this whole adventure, the biopsy was the worst of it for me. During the procedure, the urologist asked questions about my hobbies -his was carpentry- but I was too distracted to talk about airplanes.
Stage 4 is indicated by histology and backed up by the PET scan revealing radioactive (avid) spots outside of the prostate. Thankfully, this time around nothing was found in the head & neck, chest, prostate or bones. That was good news.
However, the PET/CT scan did show the presence of 5 or so avid lymph glands along the aorta from below the chest to above the prostate.
A proper prostate cancer diagnosis requires more than just a PSA value. An abnormal prostate is detected by digital examination by a urologist and the presence of cancer cells is confirmed by biopsy by a histologist.
My PSA curve.
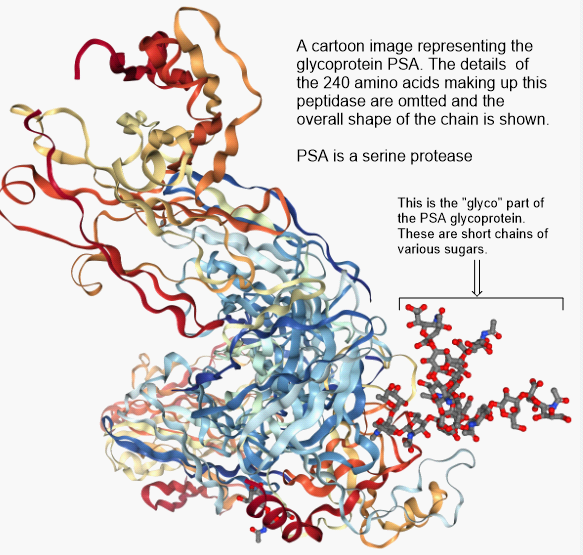
But, wait a minute. Exactly what is PSA and what does it do? According to Wikipedia, Prostate Specific Antigen (PSA) is a peptidase enzyme (a protein) secreted by the epithelial cells of the prostate gland. It’s immediate job is to liquify the semen in the seminal coagulum, allowing sperm to swim freely. It is also thought to be involved in dissolving cervical mucus, allowing sperm to enter the uterus. Amounts of PSA above a certain threshold are not normally found in the blood. Elevated PSA is associated with prostate cancer. It’s just a marker.
The glycoprotein PSA, prostate specific antigen. It is an enzyme of the serine protease variety. A protease will cleave peptide bonds in the amino acid backbone of a protein.
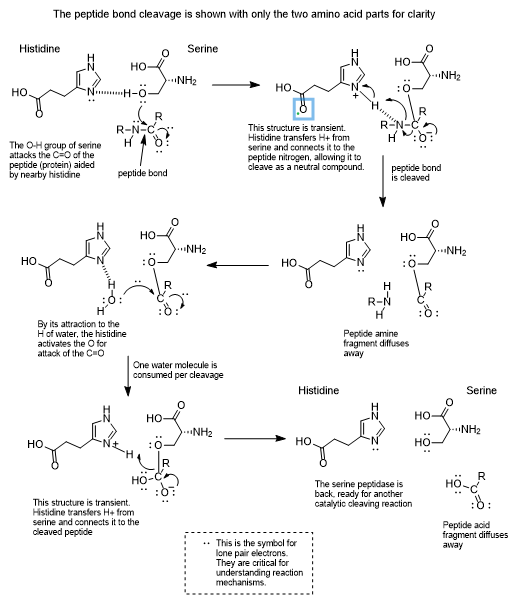
Serine protease enzymes like PSA have a serine amino acid in the active site of the enzyme which is capable of connecting temporarily with a carbonyl carbon of a (C=O) peptide bond. Since proteins are long chains of peptide bonds, cleaving a peptide bond snips the protein into smaller pieces.
Chemists are all about the mechanisms of chemical transformations and the following has been proposed for a serine protease.
All this said, it turns out that when castration resistance sets in, things begin take a turn for the worse. Prostate cancer cells begin to accumulate in the bone marrow, they begin to interact and develop into tumors that are essentially beyond the reach of treatment. The spine is a common place for them to go, but they can spread to other organs as well.
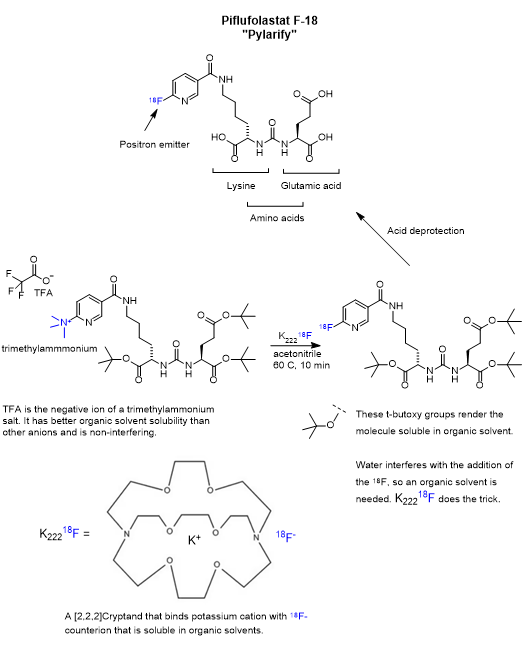
Of particular interest is the spread of prostate cancer to bone. Prostate cancer cells have an affinity for bone marrow tissue. In my case, the PET/CT scans gave no indication of being present in the head & neck, the chest or bones. That’s good news. In my first round of treatment, I was given 18F-Glucose diagnostic for the PET scan. This time I was given the more receptor-selective 18F PSMA diagnostic called Pylarify. While it is selective for a particular receptor on the cancer cell, it also shows up elsewhere in the body in the PET scan as a result of circulation and transport out of the system. Receptor-specific drugs will bind to the intended receptor, but only after they wander around and stumble into it. This is made less than random due to active transport or solubility partitioning. The effectiveness also benefits by resistance to metabolism and excretion.
Pylarify is a kind of pseudo-peptide containing two modified amino acids, lysine and glutamic acid, joined at the nitrogen atoms as a urea linkage. The key step is the nucleophilic aromatic substitution of trimethylammonium by 18F on the pyridine ring. The presence of abundant heteroatoms (nitrogen and oxygen) groups is not uncommon for pharmaceuticals and is absolutely ordinary for proteins. Heteroatoms serve as hydrogen bond donors and acceptors which is critical in biochemical transformations. A hydrogen bond donor can reversibly bind to a hydrogen bond acceptor and keep the molecules in close proximity long enough for a transformation as well as participate in it.
Sarah Piron, Jeroen Verhoeven, Christian Vanhove, Filip De Vos, Recent advancements in 18F-labeled PSMA targeting PET radiopharmaceuticals, Nuclear Medicine and Biology, Volumes 106–107, 2022, Pages 29-51, ISSN 0969-8051, https://doi.org/10.1016/j.nucmedbio.2021.12.005.
Prologue: What follows is a look at the use of 68Gallium as part of a positron emitting radioligand from an organometallic chemist’s point of view. I’m not from nuclear medicine nor am I a radiation oncologist.
It had to happen … the other shoe has dropped. My stage-4 prostate cancer has come charging back for round 2 after 9 years. Again, I’ve taken a personal interest in radiation oncology. Recently, my PSA shot up steeply through the 4.0 ng/dL threshold triggering an appointment with my radiation oncologist who has ordered a PET/CT scan. Back in 2015 I finished 18 months of hormone ablation (chemical castration) and got the PSA from 29 down to 0.01 with Lupron injections and earlier, a large cumulative dose of x-radiation in the lower abdomen. I have to say that while I experienced no discomfort at all in this round of treatment, I did lose body hair and muscle mass.
PET/CT scanning is an important tool in locating prostate cancer cells. Riding the platform in and out of the scanner is expensive but important. Unfortunately for me, the CT contrast agent is a potent emetic so the scanner becomes an expensive vomitorium ride.
The story of PET, Positron Emission Tomography, has evolved over decades of advancement. To begin, tomography, detectors and computers had to be invented. Separately, positron emission as a medically viable radiation source had to be identified and validated. A substrate for selective delivery of the isotope must be found. In the case of 18Fluorine, it is available as an organofluorine molecule like 18F-Glucose. It turns out that the 18F-Glucose concentrates in clinically useful places and K18F does not.
Positron Emitters
Atomic nuclei that are deficient in neutrons can have an instability leading to emission of a positron (anti-electron with a + charge), also called a β+ decay, which lessens the neutron deficiency by ejecting a positive charge from the nucleus. When a positron is ejected from the nucleus it finds itself immediately swarmed by the electron clouds of surrounding atoms and molecules and doesn’t travel very far. When a positron encounters a negatron (regular electron, β−), they annihilate one another and emit two gamma photons of 511 keV energy at 180 degrees apart. This is a mass to energy conversion. Loss of one positive charge from the nucleus gives rise to a transmutation of the atom causing a one-unit drop in atomic number, that is it goes from n+ to (n – 1)+, but retains most of its atomic weight. In this case, 6831Gallium undergoes positron decay to 6830Zinc.
Positron emitters include 11Carbon (T1⁄2 = 20.4 min), 13nitrogen (T1⁄2 = 10 min), 15oxygen (T1⁄2 = 2 min), 18fluorine (T1⁄2 = 110 min), 64copper, 68gallium, 78bromine, 82rubidium, 86yttrium, 89zirconium, 22sodium, 26aluminium, 40potassium, 83strontium, and 124iodine. This a list given by Wikipedia, but there are many more in more comprehensive tables.
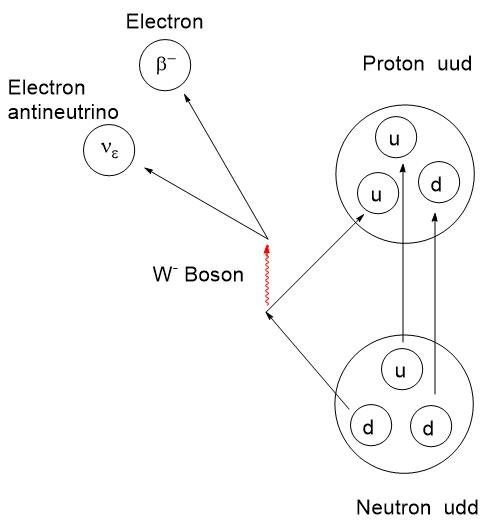
The actual mechanism of β-type emission requires a venture into fundamental particles called quarks. Protons and neutrons are composite particles called hadrons, not fundamental particles. Protons and neutrons are each comprised of 3 quarks, but with a different combination of “up and down flavors” where flavor refers to the species of quark. There are 6 flavors of quarks: up, down, charm, strange, top, and bottom. Interconversion between protons and neutrons can occur if one of the 3 top or bottom quarks changes flavor. By all means, if this interests you, take a dive into it. I shall stop here.
Beta emission diagram at quark level.
Positron emitters tend to have a short radioactive half-life as well as a limited chemical half-life in the body before they are cleared out through the kidneys or other routes. Ideally, the goal is to deliver a high radiation dose selectively to a target tissue as fast as is safe then disappear. Prolonged irradiation to surrounding tissue is undesirable. The optimal radiopharmaceutical will be highly target selective and have a short half-life. A selective radiopharmaceutical is one that will accumulate in a desired cell type or organ. Accumulation can be aided through simple solubility, the ability to undergo transport through a cell wall, affinity to a specific receptor and the ability to function fast enough to resist the various clearance mechanisms.
A short half-life means that the radioactivity per gram of radioisotope, specific activity in Becquerels per gram, will be at its maximum after activation. Though the radioactivity may be intense, the radiation dose can be controlled by the amount of mass administered. With radioisotopes, there are two kinds of purity to consider: Chemical purity referring to the atoms and molecules present; Radiological purity referring to the presence or absence of other radioactive isotopes. To provide maximum safety and effectiveness, the specific radioisotope with the desired decay mode should be the only source present. If your desired source is an alpha emitter, you don’t need spurious quantities of a gamma emitter present because of inadequate purification.
Economical methods of preparing positron emitters had to be addressed. To fully exploit PET for any given situation, tissue selectivity of radioligands had to be determined and selective positron radiopharmaceuticals developed. Due to the short half-life of these radioisotopes, rapid and safe methodologies to produce them by efficient nuclear transformations, isotope isolation followed by chemical synthesis had to be developed. It is important that isotope generation, isolation and attachment to a ligand be done nearby the hospital for the proper activity to reach the patient.
Positron emitter production involves a nuclear reactor for neutron activation or a cyclotron accelerating protons or deuterons in the preparation. Because both of these sources are highly destructive to organic molecules, an inorganic radioisotope is produced separately and chemically modified to produce an inorganic species that can be chelated or otherwise attached to a radiopharmaceutical. This technique evolved from simple radiography in the 1930’s to a large array of techniques and applications today. The reader is invited to take a dive into this topic.
Since my cancer experience began, a few new radiotherapies and imaging agents have landed in oncology space for prostate cancer. Recently I posted on Pluvicto PSMA (Prostate Specific Membrane Antigen) which was before I knew about my current prostate situation. PSMA is a transmembrane protein present in prostatic cells. Pluvicto uses a chelated177Lutetium beta emitter as the destructive warhead and a peptidomimetic fragment for binding to the PSMA receptor.
A Brief Interlude into Quality Factor
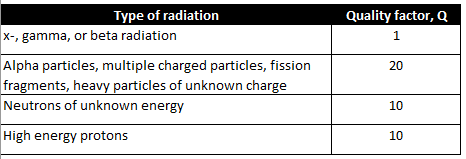
It should be noted that the various forms of particle (alpha, beta, or neutron) or electromagnetic radiation (x-ray or gamma) have differing abilities to penetrate and cause ionization of within matter. There is a factor for this which is used to refine dosage calculations. It is called the Quality factor, Q.
The destructive effects of radiation stem from its ability to ionize matter along its path. Ionization is a disruptive effect that may result in fragmentation of molecules or crystal lattices into reactive positive or negative ions. Single electron radical species may be formed as well. It is possible for some fraction of the disrupted molecules to recombine if the fragments haven’t already diffused away or gone on to further transformations.
The deleterious effects of radiation on living tissue stems from the amount of disruptive energy transferred to tissues along the path of each particle. Charged particles like electrons, protons and alpha particles tend to dump their energy into matter rapidly and along a short path making them less penetrating than neutrons or electromagnetic rays in general.
Quality factor, Q, is a dimensionless coefficient that is multiplied by an absorbed dose to give a more realistic estimation of radiation energy absorption. Interestingly, the Q for neutrons varies with energy and rises to a maximum around 0.5 to 1 MeV of energy and falls off at higher energies.
The larger the Q factor, the larger the corrected radiation effect. X-, gamma, and beta radiation have a Q factor lower than the others by a factor of 10 to 20. The x- and gamma rays will tend to pass through matter leaving a small amount of their energy to disruption. In radiation therapy this is compensated for by just increasing the fluence or the exposure time.
For clarity, x-rays are generated from the electron cloud around an atom via electron transitions. For instance, if an electron is dislodged from an inner, low energy orbital, another electron can occupy that vacancy by the emission of an x-ray. Gamma rays originate from nuclear energy transitions. Often a nuclear decay might result in a new nucleus that is not at its ground state and would be categorized as metastable. This metastable state, which has its own half-life, can collapse to its ground state by the emission of a gamma ray matching the loss of energy by the nucleus.
Neutrons
Free neutrons are special. They undergo beta decay with a short half-life outside the nucleus having t1/2 = ~ 10-15 minutes, depending on the information source. Not having a charge, they tend to be more penetrating than other particles. However, effective shielding can be had with a hydrocarbon like paraffin or water by virtue of the high concentration of hydrogen nuclei present in these substances. Neutrons are not affected by charge repulsion from an atomic nucleus and therefore can collide and interact with the hydrogen nucleus (a proton). They can scatter from hydrogen nuclei, leaving behind some of their kinetic energy with each collision (see “Neutron Lethargy“). This scattering is the basis for using water to moderate the neutrons in a nuclear reactor. Neutrons are cooled by repeated collisions with hydrogens in water to the point where their kinetic energy of 0.025 eV, which from the Maxwell-Boltzmann distribution corresponds to a temperature of 17 oC, thus the term “thermal neutrons“.
Many elements absorb neutrons, increasing the atomic weight and very often altering the stability of the nucleus leading to a radioactive decay cascade. This is what is happening in neutron activation. In the case of water, the ability of free neutrons to collide with hydrogen nuclei allows them to dislodge hydrogen ions or free radicals from organic and biomolecules resulting in ionization and makes them quite hazardous to living things.
Radioligands
Drugs like Pluvicto are referred to as a radioligand. There is a radioisotope connected to an organic “ligand” for selective binding to a specific protein receptor. A radioligand is injected and diffuses its way a particular receptor where it binds. As it turns out, due to the gamma radiation also emitted by 177Lu, Pluvicto is a radioligand that can also be located in the body by the gamma radiation it emits. In general, a radioligand can be used for two endpoints: To find and signal the location of a particular cell type; and to find and vigorously irradiate a particular cell type.
There are recent radioligand compounds that are used as PET (Positron Emission Tomography) diagnostic agents which selectively bind to the PSMA receptor where they can undergo positron emission revealing the site of prostate cancer cells by tomography. 18F-glucose was first synthesized in 1967 in Czechoslovakia at Charles University by Dr. Josef Pacák and was first tested as a radiotracer by Abass Alavi in 1976 at the University of Pennsylvania on volunteers. Positron tomography came along later. Cancer cells consume glucose faster than normal cells so the 18F will tend to accumulate to a slightly greater extent and reveal their position by positron annihilation. The two 511 keV x-rays simultaneously detected at 180o apart are identified by a ring coincidence detector. A single detection event is discarded.
Dr. Abass Alavi, University of Pennsylvania. First use of 18F-Glucose on humans.
Dr. Josef Pacák (1927-2010), of Charles University in Czechoslovakia. First to prepare 18F-Glucose.
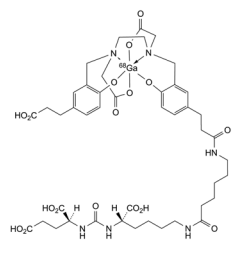
A radioligand that received FDA approval the same day as Pluvicto was Locametz or Gallium (68Ga) gozetotide. This gallium radioligand targets PSMA as does Pluvicto but is only a PET diagnostic agent.
Locametz or Gallium (68Ga) gozetotide. Source: Pharmeuropa.
Locametz has 4 carboxylic acid groups, a urea group and two amide groups aiding water solubility and numerous sites for hydrogen bonding of this radioligand to the receptor. The organic portion of the Locametz is called gozetotide, named “acyclic radiometal chelator N,N’-bis [2-hydroxy-5-(carboxyethyl)-benzyl] ethylenediamine-N,N’-diacetic acid (HBED-CC).” The 68Ga (3+) cation is shown within an octahedral complex with a single hexadentate ligand wrapping around it. The short 68 minute half-life of 68Ga requires that a nuclear pharmacy be nearby to prepare it. The short half-life of 68Ga or other positron emitters as well as the possibility of destructive radiolysis to the ligand prevents preparing a large batch and stocking it. Locametz must be synthesized and transported prior to use. This rules out remote or rural hospitals.
Nuclear Chemistry
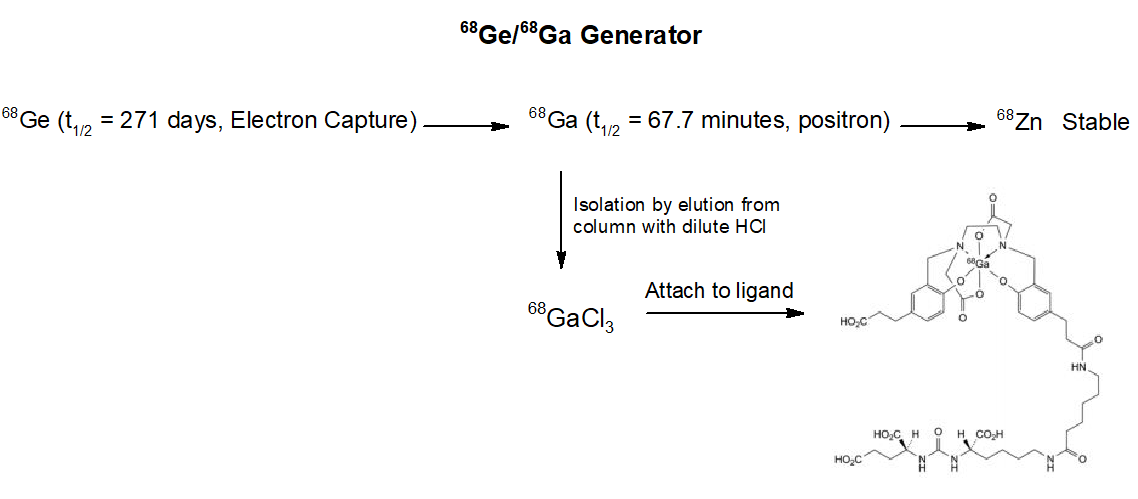
So, where does one obtain 68Gallium? Well, there are several methods out there. 68Ge/68Ga generators are produced commercially. One company is GeGantTM who offers 1-4 GBq of 68Ga. (Note: 1 GBq is 1,000,000,000 disintegrations per second).
Diagram courtesy of Gaussling.
From the scheme above we see the workings of a 68Ga generator. The ligand attachment is performed exterior to the generator. Atomic nuclei that are neutron deficient like 68Germanium can transform a proton to a neutron. There are two ways this can happen. In Electron Capture (EC) an inner “s” electron can be absorbed by a proton converting it to a neutron and emitting a neutrino by the weak nuclear force. This lowers the atomic number by 1, in this case 6832Germanium becomes 6831Gallium. The other mechanism is for the nucleus to emit a positron (anti-electron) and eject 1 positive charge as a positron (and an antineutrino) from the nucleus, resulting in a new neutron. The atomic weight remains constant, but the atomic number drops by one. If available energy in the nucleus is less than about 1 MeV, an electron capture is more favorable than positron emission.
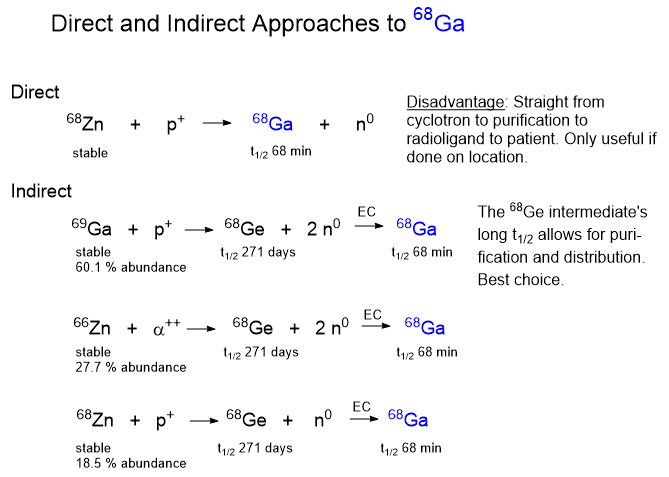
Once you know about the 68Ge electron capture reaction leading to the 68Ga isotope you have to ask, where does the 68Germanium come from? There are a few different ways to make and concentrate 68Ge and the method you use depends on the equipment available to you. One way is to accelerate protons to a high energy in a cyclotron and slam them into atoms heavier than germanium, such as rubidium or molybdenum. The collision with break the target nuclei into pieces by a process called “spallation“.
Diagram courtesy of Gaussling.
Cyclotrons
The first cyclotron was independently invented by Ernest Lawrence 1929-1930 at UC Berkeley. It was the first cyclic particle accelerator built. The idea of the cyclic accelerator was first conceived by German physicist Max Steenbeck in 1927. In 1928-1929 Hungarian physicist Leo Szilard filed patent applications for a linear accelerator, cyclotron, and the betatron for accelerating electrons. Unfortunately for both Steenbeck and Szilard, their ideas were never published or patented so word of the ideas were never made public.
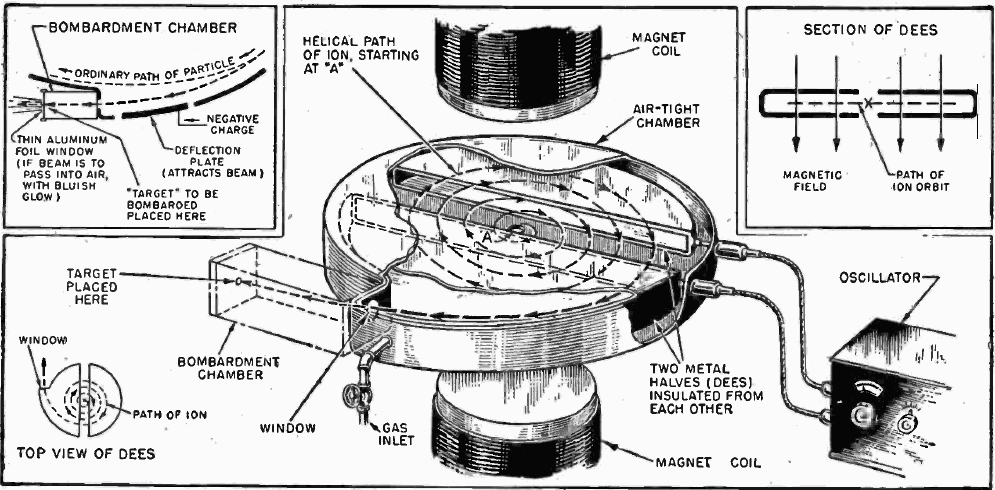
Where does one go to get a cyclotron? One company is Best Cyclotron Systems. If you are not sure of how a cyclotron works, check out the image below from Wikipedia. Note: A cyclotron can only accelerate charged particles like protons, electrons, deuterons and alpha particles which are introduced into the middle of the machine. A key component is the “D” or Dee, so-called because of their D-shape. The cyclotron has two hollow, coplanar Dees which are each connected to a high voltage radiofrequency generator. The Dees are open chamber-shaped electrodes that alternately cycle through positive and negative high voltage attracting and repelling charged particles under the influence of a powerful magnet. Because charged particles change their trajectory under the influence of a magnetic field, the particles follow a curved path of increasing diameter, accelerating until they exit the Dees and careen into the target.
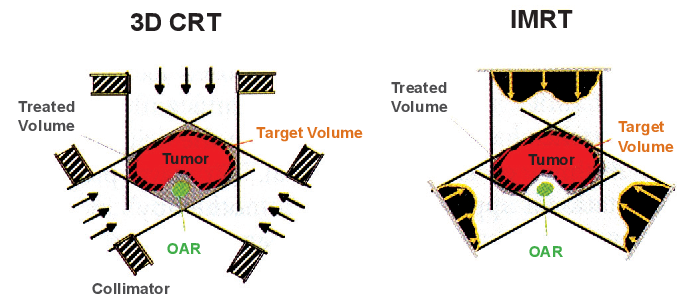
It has been right at 10 1/2 years since I was treated for squamous cell throat cancer. This virally induced cancer is quite treatable with a high success rate. The treatment was simultaneous radiation and cisplatin. The x-radiation dose was 68 Gray in daily 2 Gray doses with 6 cisplatin infusions. The radiotherapy machine was an Intensity Modulated Radiation Therapy (IMRT). The source rotates around the stationary patient varying the beam size and intensity as it goes. The idea is to put the energy into the tumor and spare healthy tissue to the greatest extent possible. The neck is a very crowded place with many kinds of tissues you don’t want to zap too much.
Illustration showing variable intensity beam shaping from the IMRT on the right. Source: Semantic Scholar.
It took about 1 week for the radiation effects to show up. It began with a sore throat which quickly led to a stomach feeding tube. They snake a pointy-ended tube down your throat and poke it out of your belly. I had it in for about 6 weeks. I jammed my liquid food in with a 60 mL syringe.
Besides the considerable discomfort from the radiation, long term side effects were not terrible. My thyroid took a big hit as did my salivary glands and taste buds. Ten years of dry mouth has led to the loss of some teeth. And, there was difficulty in swallowing initially. This problem unexpectedly returned during my recent bout of pneumonia.
The cisplatin was given in 6 doses. The nursing staff in the infusion suite don considerable PPE while handling chemotherapeutic drugs due to the toxicity hazard. I had no noticeable symptoms from this treatment. But while in the infusion suite, I could hear numerous female patients who were groaning in misery and vomiting from their meds. It was heart wrenching.
Nine years ago I wrapped up radiation for my stage 4 prostate cancer. Though the dose was lower at 38 Gray, there were no real negative effects as with the throat radiation. This was followed by 2 years of chemical castration with Lupron. It is also called hormone ablation. Lupron interferes with the production of testosterone. It does not, however prevent the adrenal glands from producing it, but this is a minor source. The first effective treatment for prostate cancer was surgical castration done to halt testosterone production. This hormone accelerates the growth and spread of the cancer. These guys who take testosterone for body building have no idea about the other thing the hormone can do. Just my opinion.
Hormone ablation eventually becomes ineffective because over time the prostate cancer cells respond by increasing the number of androgen receptor proteins on the cell walls. After hormone ablation fails, more severe treatments are put into use.
My outlook is this- The throat cancer is unlikely to return, but the prostate cancer will eventually take me out. I’ve had plenty of time to ponder death since the cancer diagnoses. I’d much prefer to have a quick, fatal heart attack than a slow, wasting death from cancer. I jokingly mentioned this to my cardiologist. He replied that the heart attack might not kill me. Buzzkill.
March 22, 2022. Swiss drugmaker Novartis has released Pluvicto, “the first FDA-approved targeted radioligand therapy (RLT) for eligible patients with mCRPC that combines a targeting compound (ligand) with a therapeutic radioisotope (a radioactive particle). Pluvicto is expected to be available to physicians and patients within weeks.“
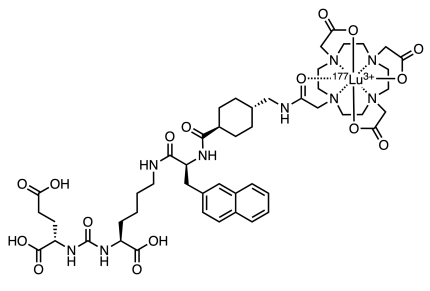
Pluvicto features a chelated Lutetium-177 ion (half-life 6.7 days) which is the source of the molecule’s radioactivity. Lutetium is the heaviest of the lanthanide elements and the name comes from the Latin Lutetia Parisiorum which was the predecessor to the city of Paris, France.
The drug has been approved in the US for the treatment of metastatic prostate cancer. Several things are notable about the Pluvicto molecule. The molecule contains a PSMA-specific peptidomimetic feature with an attached therapeutic radionuclide, where PSMA stands for Prostate Specific Membrane Antigen. Peptidomimetic refers to a small chain that resembles a stretch of protein forming amino acids. This peptidomimetic fragment, which interestingly contains a urea linker, is designed as the tumor targeting piece of the drug. Connected to it is a radioactive Lutetium-177 cation (below, upper right). The tumor targeting fragment binds to the cancer cell. While bound to the cell, the short-lived radioisotope undergoes two modes of decay. The Lu-177 emits a medium energy beta particle (Eβmax = 0.497 MeV) which is limited to a maximum of 2 millimeters of travel. This is the kill shot that will damage the attached target cell. The short path length of the beta ray in vivo limits the extent of surrounding damage by any given decay.
The other mode of decay is gamma emission by Lu-177. Gamma rays are much more penetrating than beta particles. They can be detected from the exterior allowing monitoring of dose and location of the drug. Even though gamma rays are more penetrating than beta rays, they produce many fewer ion pairs per centimeter as they traverse the tissue making them less effective in tissue destruction compared to alpha and beta particles. For instance alpha particles from therapeutic radionuclides like Radium-223 use to treat prostate cancer are much more destructive because they produce many ion pairs per centimeter. This is why getting alpha emitters like radon inside you is not a good thing.
A Google search of Pluvicto or Lutetium-177 will produce many good links of a technical and non-technical nature.
Pluvicto, PSMA-targeted radiotherapy (lutetium 177Lu vipivotide tetraxetan) for PSMA-positive prostate cancer 7.4 GBq (200 mCi) IV Q6W up to 6 doses
Novartis PluvictoTM (lutetium Lu 177 vipivotide tetraxetan)